

The relationship between sleep-disordered breathing, blood pressure, and urinary cortisol and catecholamines in children
- PMID: 32043963
- PMCID: PMC7849664
- DOI: 10.5664/jcsm.8360
The relationship between sleep-disordered breathing, blood pressure, and urinary cortisol and catecholamines in children
Abstract
Study objectives: Hypertension is a complication of obstructive sleep apnea (OSA) syndrome in adults. A correlation between OSA syndrome and elevated blood pressure (BP) is suggested in children, but its pathogenesis remains unclear. Our aim was to study the effects of sleep and sleep apnea on BP and sympathetic nervous system activation as measured by serum cortisol and urinary catecholamines. We hypothesized that children with OSA syndrome would have higher BP, urinary catecholamines, and cortisol compared with controls.
Methods: We measured BP during polysomnography in 78 children with suspected sleep-disordered breathing and 18 nonsnoring controls. BP was measured during wakefulness and every 30-60 minutes throughout the night. All participants had 24-hour urinary catecholamine and free cortisol collections 48 hours before polysomnography.
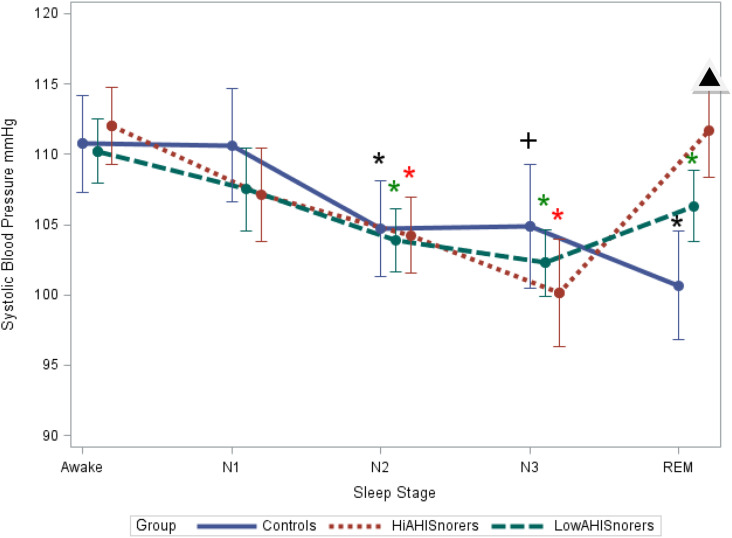
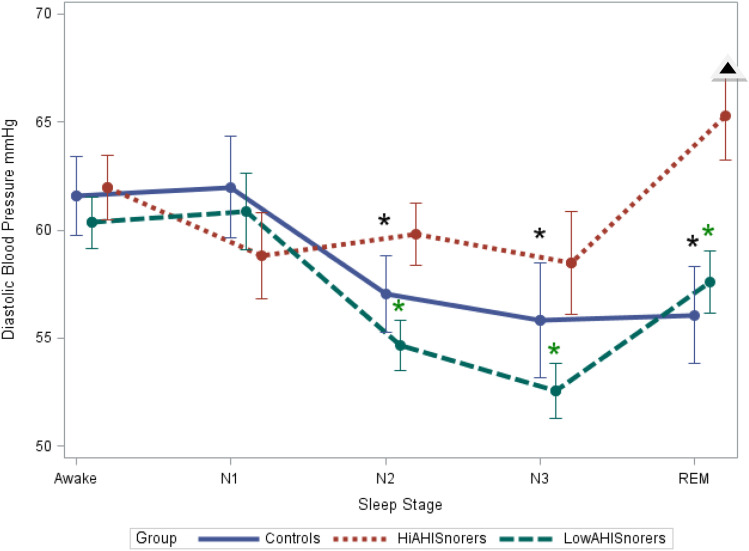
Results: BP varied with sleep stage; it was highest during wakefulness and N1 and lowest during non-rapid eye movement stage 3. Children classified as high apnea-hypopnea index (AHI) snorers (AHI >5 events/h) had a greater prevalence of systolic hypertension (57%) than low-AHI snorers (22%) and nonsnoring controls (22%; P = .04). The high-AHI snorers also had higher diastolic BP (P < .02) as well as blunted nocturnal diastolic BP changes during sleep (P = .02) compared with low-AHI snorers (AHI <5 events/h). Twenty-hour urinary free cortisol and 24-hour urinary catecholamines were not associated with BP.
Conclusions: BP in children varies with sleep stage. OSA is associated with systolic hypertension, higher BP during rapid eye movement sleep, as well as elevation of diastolic BP and blunted BP changes with sleep.
Keywords: blood pressure; catecholamines; children; cortisol; hypertension; obstructive sleep apnea.
© 2020 American Academy of Sleep Medicine.
Conflict of interest statement
The authors have seen and approved the manuscript. Work for this study was performed at the Children’s Hospital of Philadelphia, Philadelphia, Pennsylvania. This study was funded by grants K-23-RR021973 (A.K.) and HL58585 (C.L.M.), an Institutional Clinical and Translational Science Award Research Grant (UL1-RR-024134) from the National Center for Research Resources, P30 AG028747 (J.D.S.), and P30 DK072488 (J.D.S.).
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
