

Side-effects profile and outcomes of ponatinib in the treatment of chronic myeloid leukemia
- PMID: 32045474
- PMCID: PMC7013263
- DOI: 10.1182/bloodadvances.2019000268
Side-effects profile and outcomes of ponatinib in the treatment of chronic myeloid leukemia
Abstract
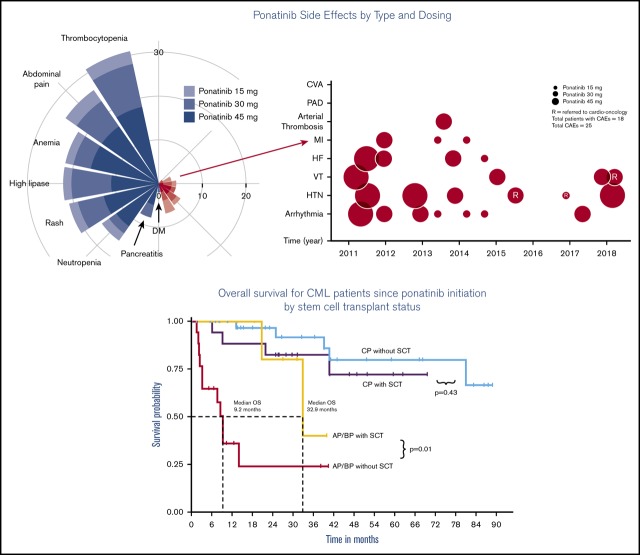
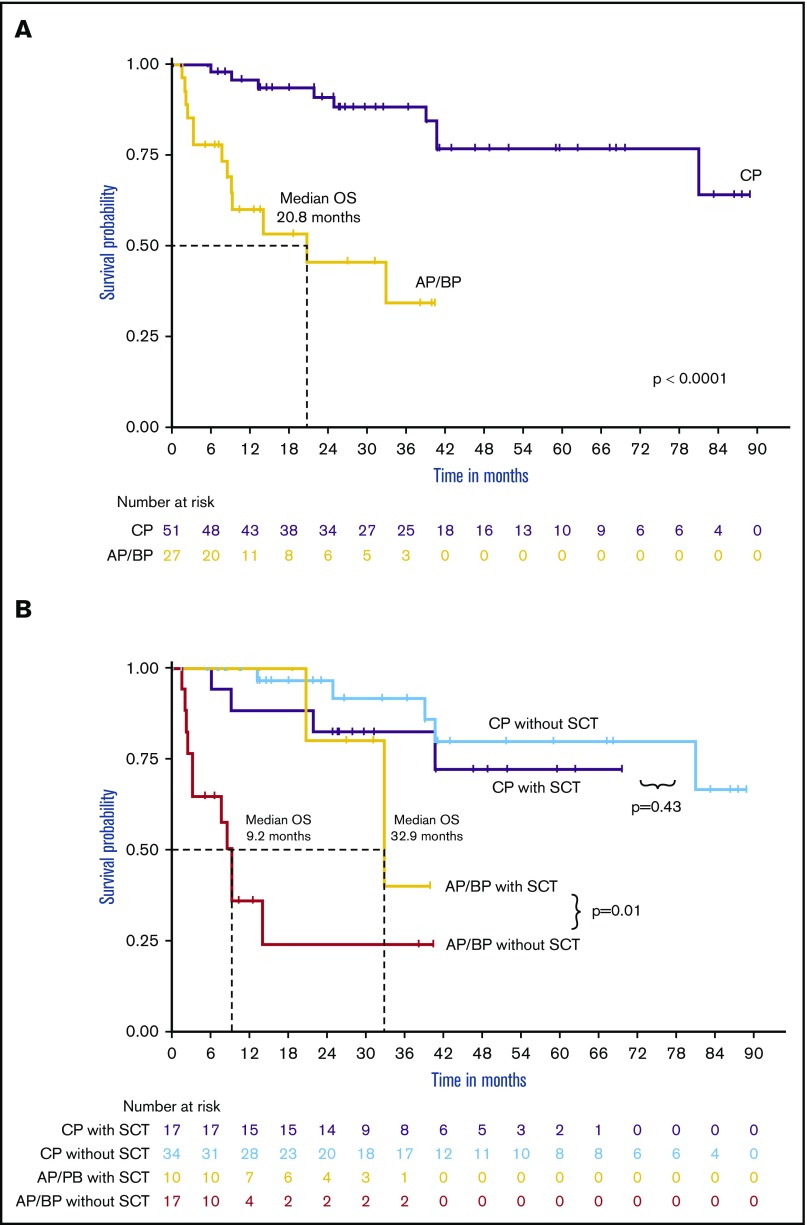
Ponatinib is associated with cardiovascular adverse events (CAEs), and its frequency in the real world is limited. In this retrospective study, we examined the survival outcomes and associated toxicities in 78 consecutive ponatinib-treated patients with chronic myeloid leukemia (CML) at the Moffitt Cancer Center from January 2011 through December 2017. The most common non-CAE was thrombocytopenia (39.7%), occurring in a dose-dependent fashion. Eighteen patients (23.1%) experienced some form of CAE, with the most common being arrhythmia (9%) and hypertension (7.7%), whereas 3 patients experienced myocardial infarction (3.8%). Before 2014, most patients were started on ponatinib 45 mg daily. There was an inverse correlation between cardio-oncology referral and the number of CAEs (P = .0440); however, a lower ponatinib starting dose, more frequent dose reduction, and increased cardio-oncology referral all were likely to have contributed to the observed decrease in CAEs after 2014. The response rate and 5-year overall survival (OS) were higher than those observed in the Ponatinib Ph+ ALL and CML Evaluation (PACE) trial (major molecular response, 58.7% vs 40% and OS, 76% vs 73%; median follow-up of 32.5 months). Ponatinib-treated patients with chronic phase-CML did not show a significant improvement with allogeneic stem cell transplantation, whereas those with accelerated phase/blast phase-CML had a much better outcome (median OS of 32.9 months vs 9.2 months; P = .01). These results demonstrate that ponatinib is highly effective. Dose adjustments and increased awareness of the cardiotoxicities associated with ponatinib may help maximize its benefits.
© 2020 by The American Society of Hematology.
Conflict of interest statement
Conflict-of-interest disclosure: J.P.-I. has received honoraria for consulting from Novartis and Bristol-Myers Squibb and is on the speakers bureau of Takeda. K.S. has received honoraria from Novartis for consulting and is on its speakers bureau. L.N. is on the speakers bureau of Novartis and has received a consulting fee from Pfizer. M.F. has received honoraria from Novartis for consulting. The remaining authors declare no competing financial interests.
Figures


Comment in
-
Poor tolerability to ponatinib in Indian CML patients.Blood Adv. 2020 May 12;4(9):1927-1929. doi: 10.1182/bloodadvances.2020001944. Blood Adv. 2020. PMID: 32380534 Free PMC article. No abstract available.
References
-
- de Klein A, van Kessel AG, Grosveld G, et al. A cellular oncogene is translocated to the Philadelphia chromosome in chronic myelocytic leukaemia. Nature. 1982;300(5894):765-767. - PubMed
-
- Baccarani M, Castagnetti F, Gugliotta G, Rosti G. A review of the European LeukemiaNet recommendations for the management of CML. Ann Hematol. 2015;94(suppl 2):141-147. - PubMed
-
- Talati C, Pinilla-Ibarz J. Resistance in chronic myeloid leukemia: definitions and novel therapeutic agents. Curr Opin Hematol. 2018;25(2):154-161. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
