

Best Practices Guideline for the Pathologic Diagnosis of Breast Implant-Associated Anaplastic Large-Cell Lymphoma
- PMID: 32045544
- PMCID: PMC7106983
- DOI: 10.1200/JCO.19.02778
Best Practices Guideline for the Pathologic Diagnosis of Breast Implant-Associated Anaplastic Large-Cell Lymphoma
Abstract
Purpose: To provide guidelines for the accurate pathologic diagnosis of breast implant-associated anaplastic large cell lymphoma (BIA-ALCL), the preoperative evaluation of the patient with suspected BIA-ALCL, and the pathologic evaluation of the capsulectomy specimen.
Methods: To better inform patients and healthcare providers about BIA-ALCL, we convened to review diagnostic procedures used in the evaluation of patients with suspected BIA-ALCL. We focused on the processing of the seroma fluid/effusion surrounding the implant, the handling of capsulectomy specimens following removal of implant(s), and the preoperative evaluation of the patient with suspected BIA-ALCL. Recommendations were based on the published literature and our experience to optimize procedures to obtain an accurate diagnosis and assess for tumor invasion and the extent of the disease.
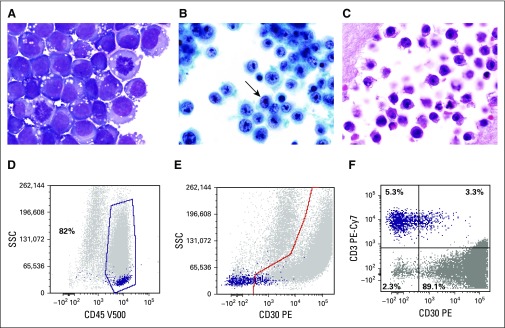
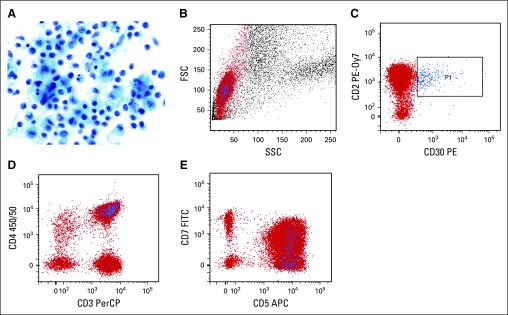
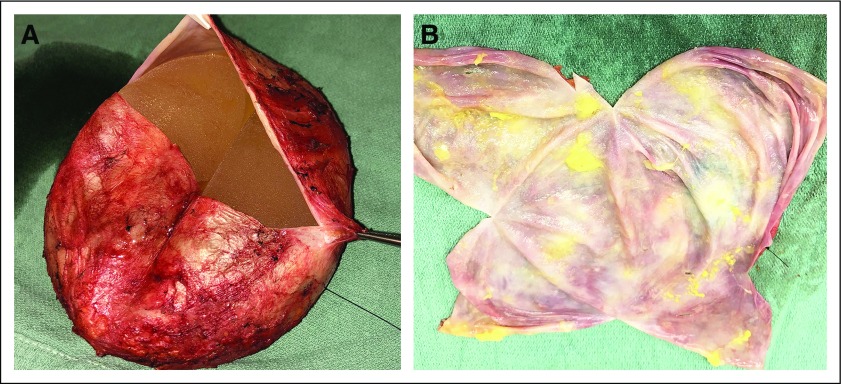
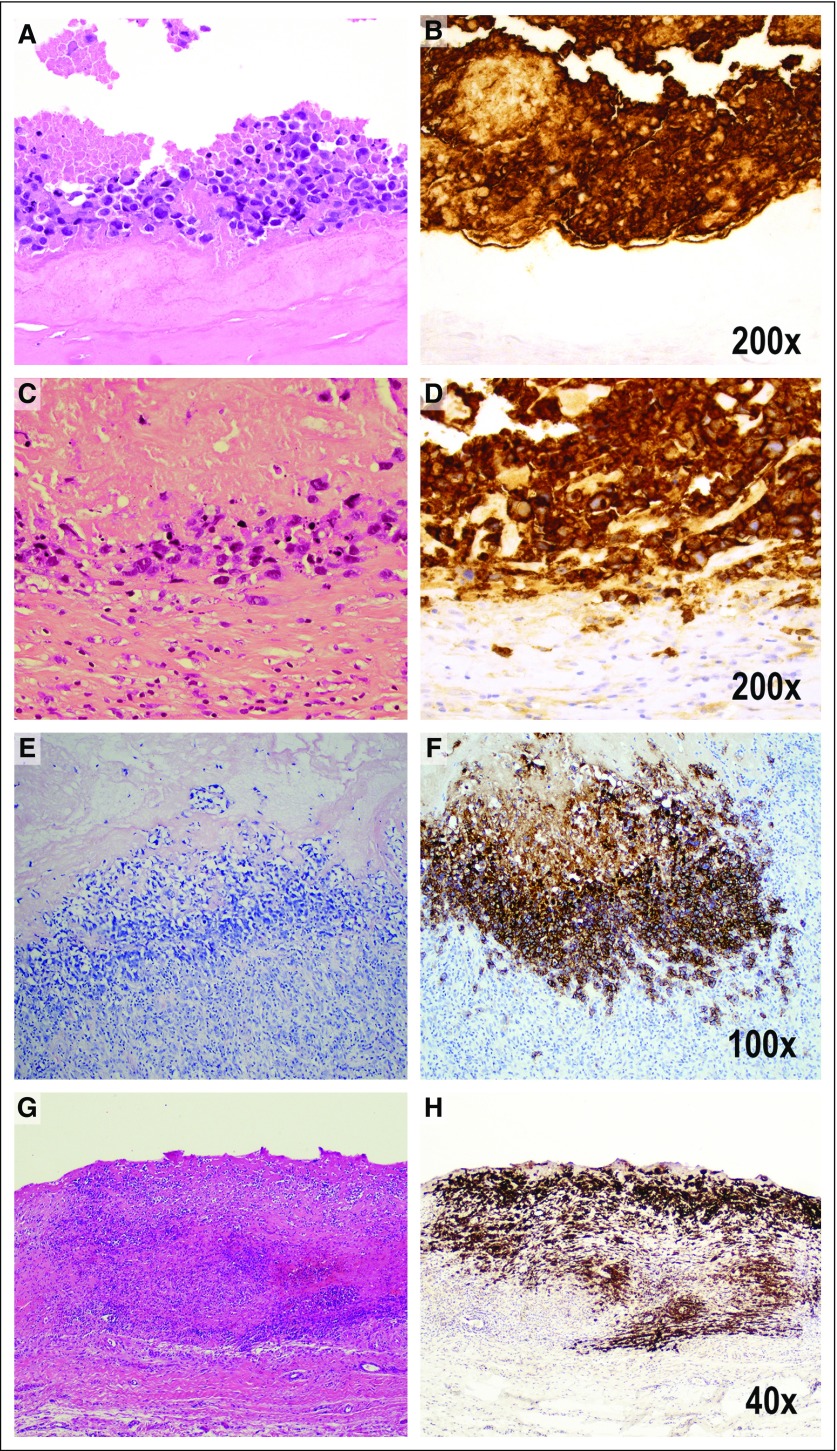
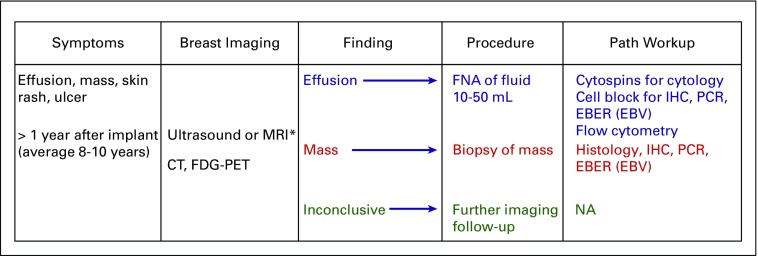
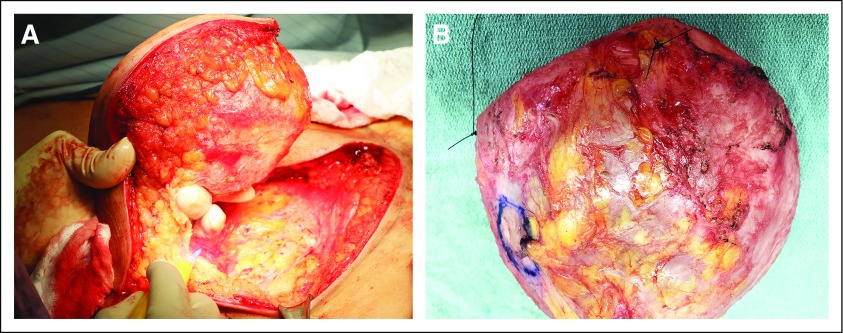
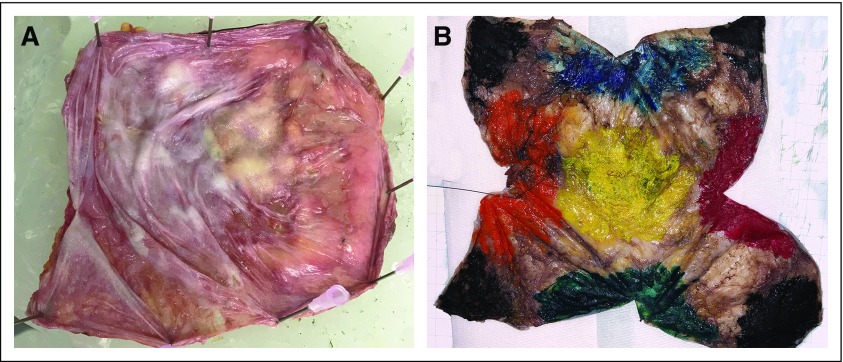
Recommendations: Early diagnosis of BIA-ALCL is important as the disease can progress and deaths have been reported. Because the most common presentation of BIA-ALCL is swelling of the breast with fluid collection, an accurate diagnosis requires cytologic evaluation of the effusion fluid surrounding the affected implant. The first priority is cytocentrifugation and filtration of fresh, unfixed effusion fluid to produce air-dried smears that are stained with Wright-Giemsa or other Romanowsky-type stains. Preparation of a cell block is desirable to allow for hematoxylin and eosin staining and immunohistochemical analysis of formalin-fixed, paraffin-embedded histologic sections. Cell block sections can be used for polymerase chain reaction-based investigation of T-cell receptor gene rearrangement to detect clonality. Fixation and mapping of the capsulectomy specimen to select multiple representative sections are advised to assess for microscopic tumor involvement and capsular invasion. It is appropriate to assess lymph node involvement by excisional biopsy material rather than fine needle aspiration, due to propensity for focal involvement.
Figures
Comment in
-
Reply to M. Romero et al.J Clin Oncol. 2020 Aug 20;38(24):2819-2820. doi: 10.1200/JCO.20.00931. Epub 2020 Jun 17. J Clin Oncol. 2020. PMID: 32552469 Free PMC article. No abstract available.
-
Should Flow Cytometry Be Considered a First Line of Study in the Diagnosis of Breast Implant-Associated Anaplastic Large-Cell Lymphoma?J Clin Oncol. 2020 Aug 20;38(24):2816-2819. doi: 10.1200/JCO.20.00712. Epub 2020 Jun 17. J Clin Oncol. 2020. PMID: 32552470 No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
