

Predictors of Postoperative Seizure Outcome in Low Grade Glioma: From Volumetric Analysis to Molecular Stratification
- PMID: 32046310
- PMCID: PMC7072647
- DOI: 10.3390/cancers12020397
Predictors of Postoperative Seizure Outcome in Low Grade Glioma: From Volumetric Analysis to Molecular Stratification
Abstract
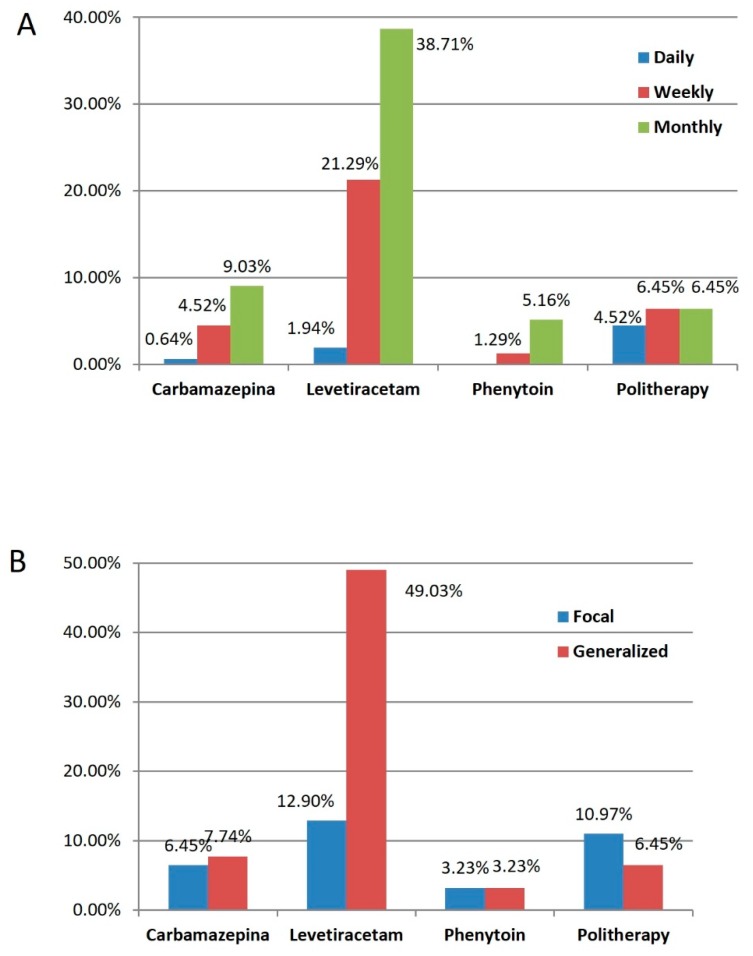
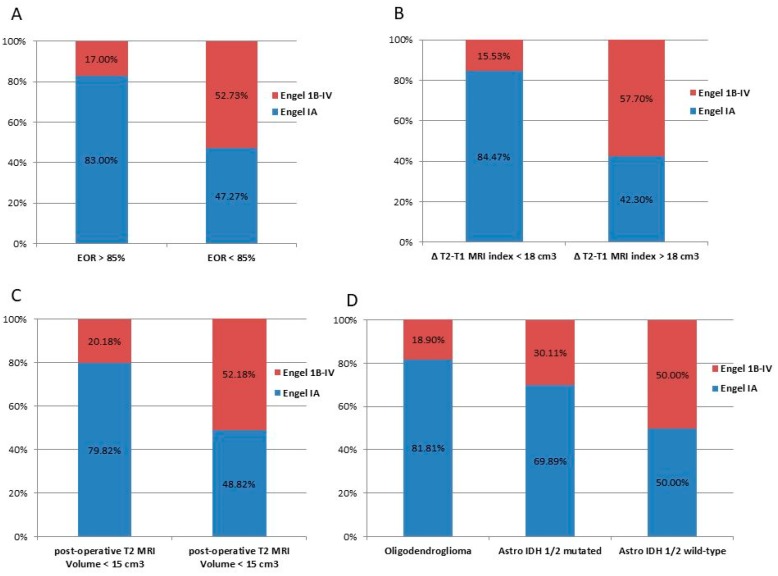
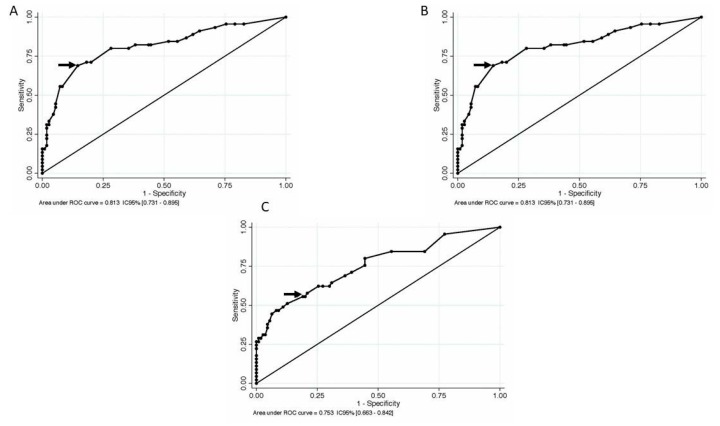
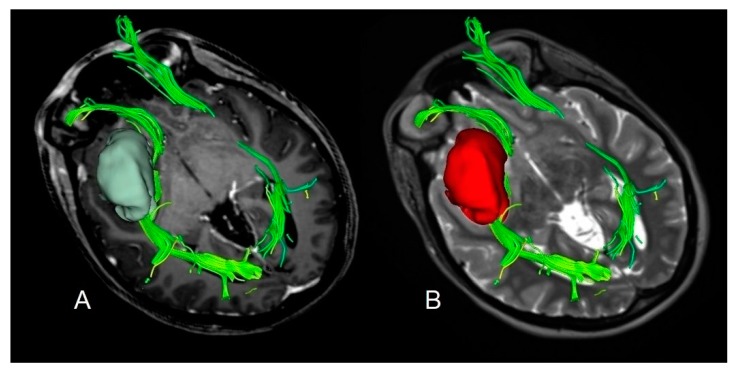
The importance of the extent of resection (EOR) has been widely demonstrated as the main predictor for survival, nevertheless its effect on tumor related epilepsy is less investigated. A total of 155 patients were enrolled after a first-line surgery for supratentorial Diffuse Low Grade Gliomas (DLGGs). Postoperative seizure outcome was analyzed stratifying the results by tumor volumetric data and molecular markers according to 2016 WHO classification. Receiver operating characteristic (ROC) curves were computed to asses EOR, residual tumor volume, and ΔT2T1 MRI index (expressing the tumor growing pattern) corresponding to optimal seizure outcome. A total of 70.97% of patients were seizure-free 18 months after surgery. Better seizure outcome was observed in IDH1/2 mutated and 1p/19q codeleted subgroup. At multivariate analysis, age (p = 0.014), EOR (p = 0.030), ΔT2T1 MRI index (p = 0.016) resulted as independent predictors of postoperative seizure control. Optimal parameters to improve postoperative seizure outcome were EOR ≥ 85%, ΔT2T1 MRI index ≤ 18 cm3, residual tumor volume ≤ 15 cm3. This study confirms the role of EOR and tumor growing pattern on postoperative seizure outcome independently from the molecular class. Higher ΔT2T1 MRI index, representing the infiltrative component of the tumor, is associated with worse seizure outcome and strengthens the evidence of common pathogenic mechanisms underlying tumor growth and postoperative seizure outcome.
Keywords: ROC curves; extent of resection; low grade glioma; molecular markers; seizure outcome; tumor growth pattern.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Aronica E., Leenstra S., van Veelen C.W., van Rijen P.C., Hulsebos T.J., Tersmette A.C., Yankaya B., Troost D. Glioneuronal tumors and medically intractable epilepsy: A clinical study with long-term follow-up of seizure outcome after surgery. Epilepsy. Res. 2001;43:179–191. doi: 10.1016/S0920-1211(00)00208-4. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
