

Evaluation of emergency obstetric and neonatal care services in Kumba Health District, Southwest region, Cameroon (2011-2014): a before-after study
- PMID: 32046673
- PMCID: PMC7014610
- DOI: 10.1186/s12884-020-2774-9
Evaluation of emergency obstetric and neonatal care services in Kumba Health District, Southwest region, Cameroon (2011-2014): a before-after study
Abstract
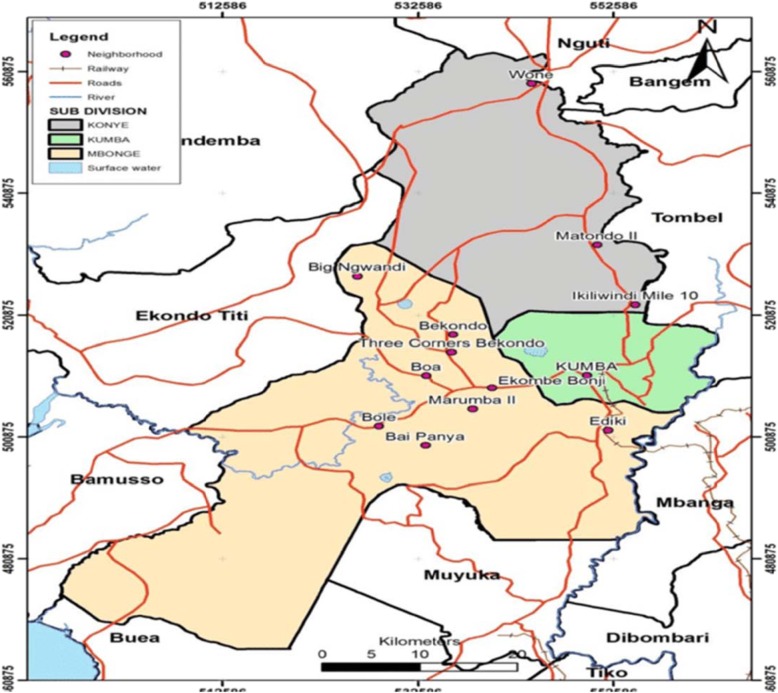
Background: There is uncertainty regarding the status of emergency obstetric and neonatal care (EmONC) in the Cameroonian context where maternal and neonatal mortality are persistently high. This study sought to evaluate the coverage, functionality and quality of EmONC services in Kumba health district (KHD), the largest health district in Southwest Cameroon..
Methods: A retrospective study of routine EmONC data for the periods 1 January 2011 to 31 December 2012 (when EmONC was being introduced) and 1 January 2013 to 31 December 2014 (when EmONC was fully instituted) was conducted. Coverage, functionality and quality of EmONC services were graded as per United Nations (UN) standards. Data was analysed using Epi-Info version 7 statistical software.
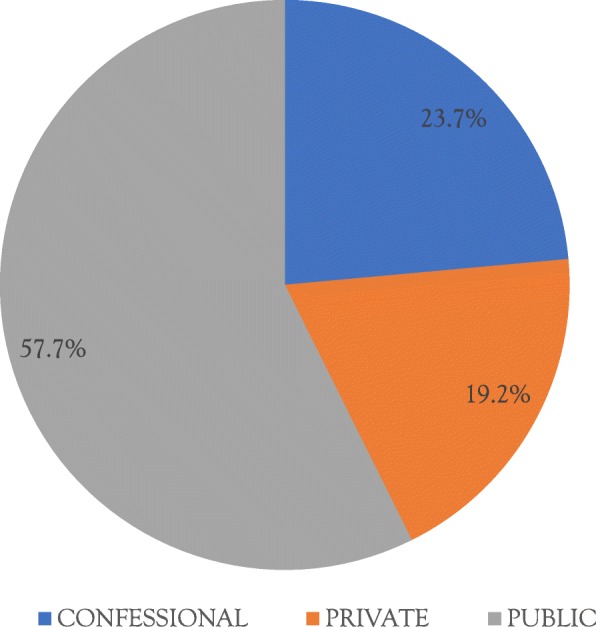
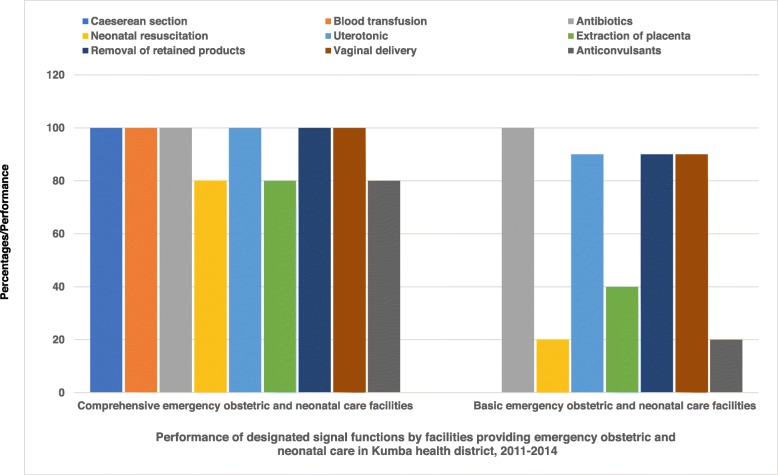
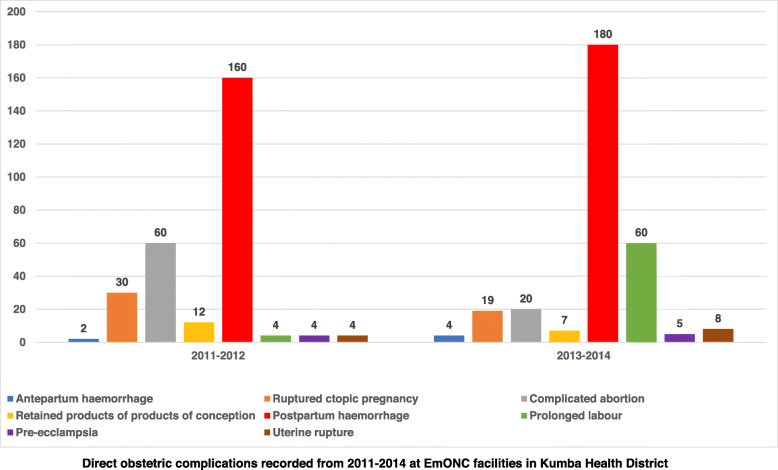
Results: Among the 31 health facilities in KHD, 12 (39%) had been delivering EmONC services. Three (25%) of these were geographically inaccessible Among the 9 facilities that were assessed, 4 facilities (44%) performed designated signal functions, with 2 being comprehensive (CEmONC) and 2 basic (BEmONC). These exceeded the required minimum of 2.8 EmONC facilities/500000, 0.6 CEmONC facilities/500000 and 2.2 BEmONC facilities/500000, with reference to an estimated KHD population of 265,071. The signal functions that were least likely to be performed were neonatal resuscitation, manual evacuation of retained products and use of anticonvulsants. In 2011-2012, the facilities performed 35% of expected deliveries. This dropped to 28% in 2013-2014. Caesarean sections as a proportion of expected deliveries remained very low: 1.5% in 2010-2011 and 3.6% in 2013-2014. In 2011-2012, met needs were 6.8% and increased to 7.3% in 2013-2014. Direct obstetric fatality rates increased from 8 to 11% (p = 0.64). Intrapartum and very early neonatal deaths increased from 4.% to 7 (p = 0.89).
Conclusion: Major gaps were observed in the performance of signal functions as well as the quality and utilization of EmONC. While the results of this study seem to indicate the need to sustainably scale up the utilization of quality EmONC, the interpretations of our findings require consideration of improvements in reporting of mortality data associated with the introduction of EmONC as well as dynamics in country-specific maternal health policies and the potential influence of these policies on EmONC indicators.
Keywords: Availability; Care; Emergency; Neonatal; Obstetric; Quality; Utilization.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Alkema Leontine, Chou Doris, Hogan Daniel, Zhang Sanqian, Moller Ann-Beth, Gemmill Alison, Fat Doris Ma, Boerma Ties, Temmerman Marleen, Mathers Colin, Say Lale. Global, regional, and national levels and trends in maternal mortality between 1990 and 2015, with scenario-based projections to 2030: a systematic analysis by the UN Maternal Mortality Estimation Inter-Agency Group. The Lancet. 2016;387(10017):462–474. doi: 10.1016/S0140-6736(15)00838-7. - DOI - PMC - PubMed
-
- World Health Organization. Trends in Maternal Mortality: 1990–2013; Estimates by WHO, UNICEF, UNFPA, The World Bank and the United Nations Population Division. Geneva: WHO; 2014.
-
- Hogan Margaret C, Foreman Kyle J, Naghavi Mohsen, Ahn Stephanie Y, Wang Mengru, Makela Susanna M, Lopez Alan D, Lozano Rafael, Murray Christopher JL. Maternal mortality for 181 countries, 1980–2008: a systematic analysis of progress towards Millennium Development Goal 5. The Lancet. 2010;375(9726):1609–1623. doi: 10.1016/S0140-6736(10)60518-1. - DOI - PubMed
-
- World Health Organization. Trends in Maternal Mortality: 1990–2015; Estimates by WHO, UNICEF, UNFPA, The World Bank and the United Nations Population Division. Geneva: WHO; 2015.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
