

Circulating Tumor DNA Analysis to Assess Risk of Progression after Long-term Response to PD-(L)1 Blockade in NSCLC
- PMID: 32046999
- PMCID: PMC7299781
- DOI: 10.1158/1078-0432.CCR-19-3418
Circulating Tumor DNA Analysis to Assess Risk of Progression after Long-term Response to PD-(L)1 Blockade in NSCLC
Abstract
Purpose: Treatment with PD-(L)1 blockade can produce remarkably durable responses in patients with non-small cell lung cancer (NSCLC). However, a significant fraction of long-term responders ultimately progress and predictors of late progression are unknown. We hypothesized that circulating tumor DNA (ctDNA) analysis of long-term responders to PD-(L)1 blockade may differentiate those who will achieve ongoing benefit from those at risk of eventual progression.
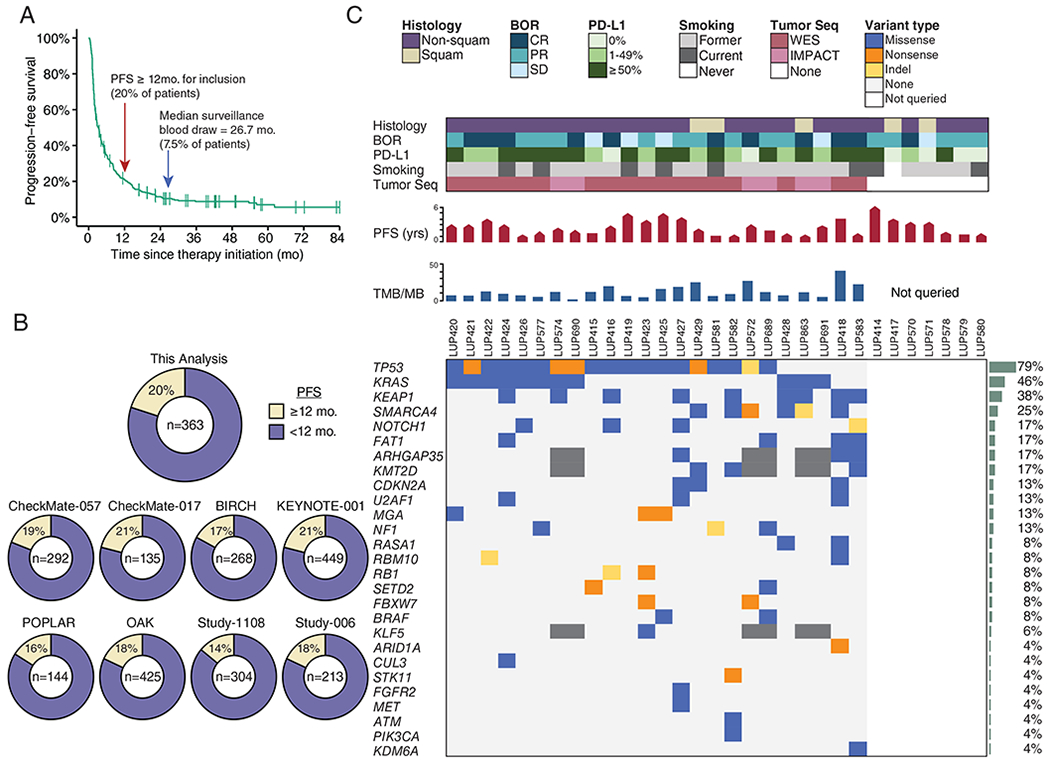
Experimental design: In patients with advanced NSCLC achieving long-term benefit from PD-(L)1 blockade (progression-free survival ≥ 12 months), plasma was collected at a surveillance timepoint late during/after treatment to interrogate ctDNA by Cancer Personalized Profiling by Deep Sequencing. Tumor tissue was available for 24 patients and was profiled by whole-exome sequencing (n = 18) or by targeted sequencing (n = 6).
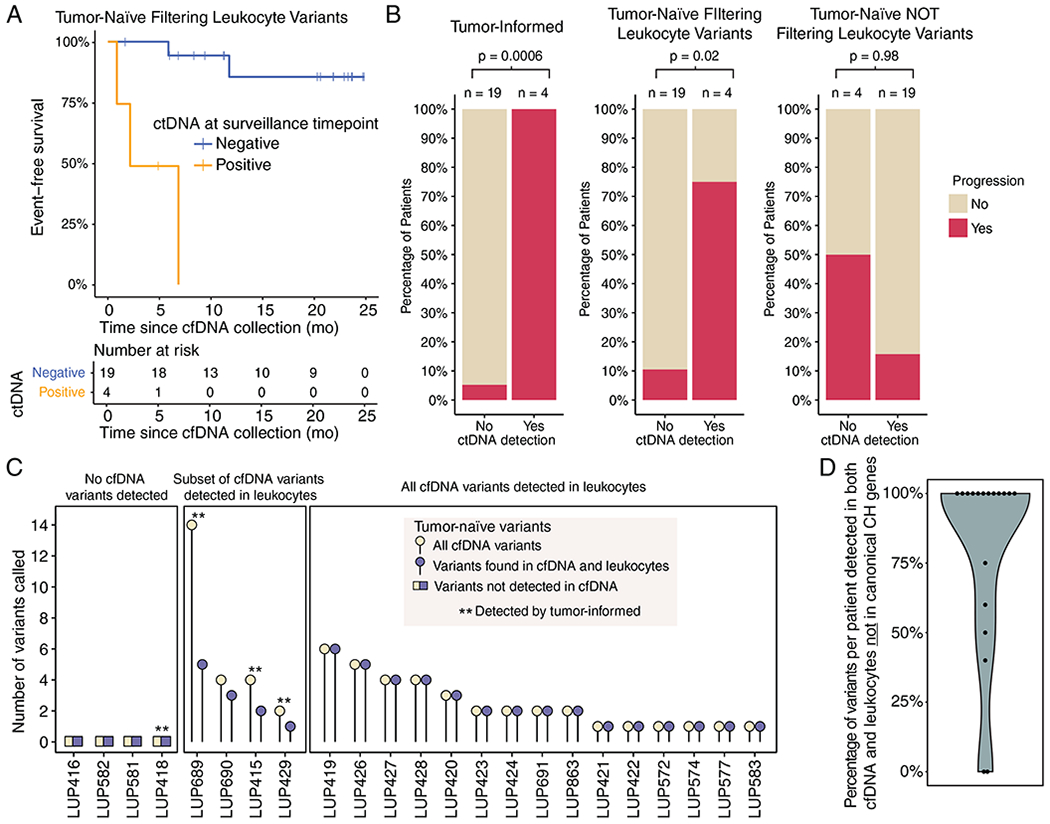
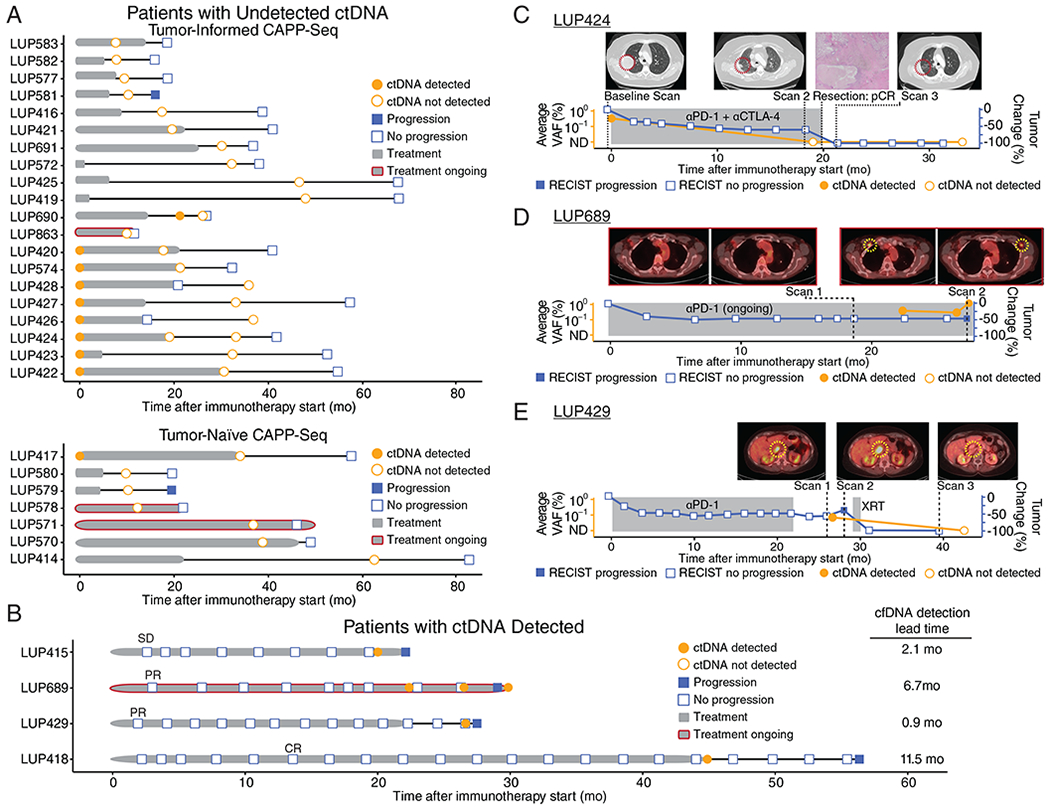
Results: Thirty-one patients with NSCLC with long-term benefit to PD-(L)1 blockade were identified, and ctDNA was analyzed in surveillance blood samples collected at a median of 26.7 months after initiation of therapy. Nine patients also had baseline plasma samples available, and all had detectable ctDNA prior to therapy initiation. At the surveillance timepoint, 27 patients had undetectable ctDNA and 25 (93%) have remained progression-free; in contrast, all 4 patients with detectable ctDNA eventually progressed [Fisher P < 0.0001; positive predictive value = 1, 95% confidence interval (CI), 0.51-1; negative predictive value = 0.93 (95% CI, 0.80-0.99)].
Conclusions: ctDNA analysis can noninvasively identify minimal residual disease in patients with long-term responses to PD-(L)1 blockade and predict the risk of eventual progression. If validated, ctDNA surveillance may facilitate personalization of the duration of immune checkpoint blockade and enable early intervention in patients at high risk for progression.
©2020 American Association for Cancer Research.
Figures

References
-
- Gandhi L, Rodríguez-Abreu D, Gadgeel S, Esteban E, Felip E, De Angelis F, et al. Pembrolizumab plus Chemotherapy in Metastatic Non–Small-Cell Lung Cancer. N Engl J Med. 2018;378:2078–92. - PubMed
-
- Reck M, Rodríguez-Abreu D, Robinson AG, Hui R, Csőszi T, Fülöp A, et al. Pembrolizumab versus Chemotherapy for PD-L1–Positive Non–Small-Cell Lung Cancer. N Engl J Med. 2016;375:1823–33. - PubMed
-
- Socinski MA, Jotte RM, Cappuzzo F, Orlandi F, Stroyakovskiy D, Nogami N, et al. Atezolizumab for First-Line Treatment of Metastatic Nonsquamous NSCLC. N Engl J Med. 2018;378:2288–301. - PubMed
-
- Gettinger S, Horn L, Jackman D, Spigel D, Antonia S, Hellmann M, et al. Five-Year Follow-Up of Nivolumab in Previously Treated Advanced Non–Small-Cell Lung Cancer: Results From the CA209–003 Study. J Clin Oncol. 2018;36:1675–84. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
