

Impact of sex and myocardial function on association of obesity with mortality in Asian patients with acute heart failure: a retrospective analysis from the STRATS-AHF registry
- PMID: 32047009
- PMCID: PMC7045129
- DOI: 10.1136/bmjopen-2019-031608
Impact of sex and myocardial function on association of obesity with mortality in Asian patients with acute heart failure: a retrospective analysis from the STRATS-AHF registry
Abstract
Objectives: Impact of sex and myocardial function on the obesity paradox in heart failure (HF) is unknown. We explored whether sex, myocardial function, and left ventricular (LV) geometry explains the protective association of body mass index (BMI) with mortality, and investigated whether metabolic health status affects this association.
Design: A multicentre cohort study with patients with acute HF admitted from January 2009 to December 2016 with a median follow-up of 33.7 months.
Setting: Three tertiary hospitals.
Participants: A total of 2021 overweight-to-obese (OW) and 1543 normal-weight (NW) patients with acute HF.
Measurements: The primary outcome was all-cause mortality. Patients were categorised as either OW (BMI≥23kg/m2) or NW (BMI<23kg/m2). BMI was used as both categorical and continuous variables. Clinical, laboratory and echocardiographic measures, including LV global longitudinal strain (LV-GLS), LV-ejection fraction, LV geometry, were obtained.
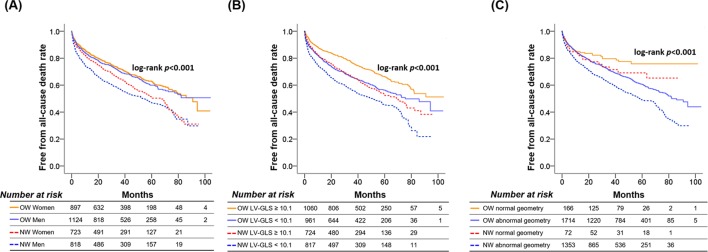
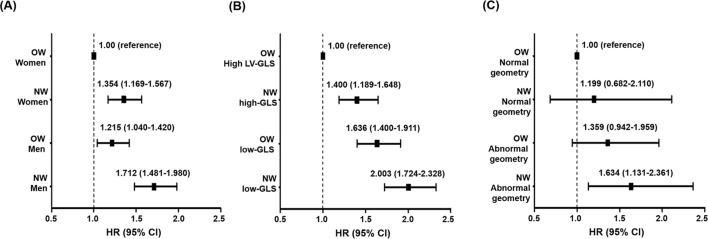
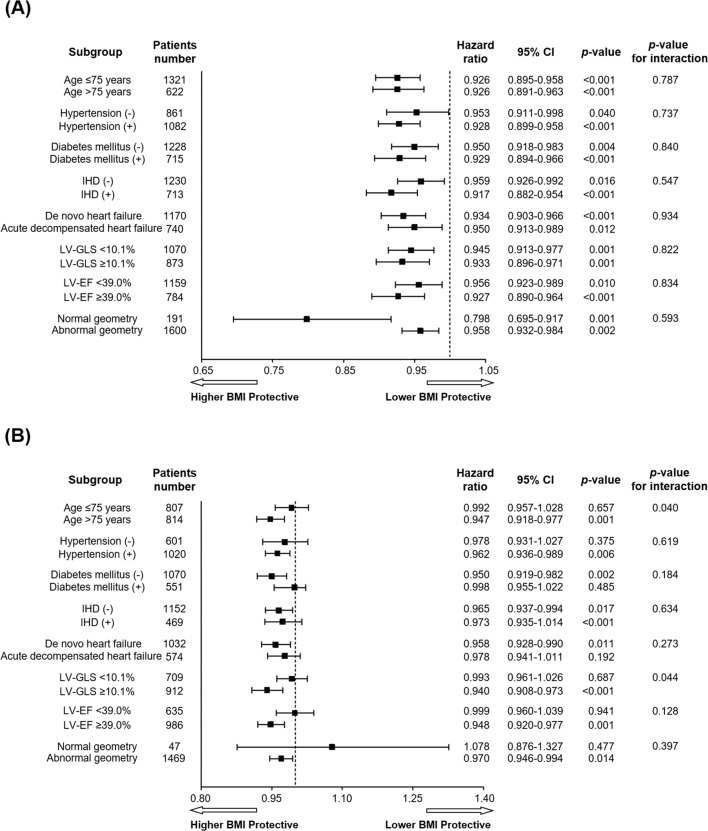
Results: During the follow-up period, 1392 patients died (685 OW and 707 NW). BMI was significantly associated with mortality in univariate (HR=0.929 per kg/m2, p<0.001) and multivariate analyses (HR=0.954 per kg/m2, p<0.001). In multivariable fractional polynomials, higher BMIs were associated with lower mortality overall and in subgroups by sex, LV-GLS and LV geometry, with a steeper association in men (p-interaction <0.001). In women, there were significant interactions of BMI with LV-GLS (p-interaction=0.044) and age (p-interaction=0.040) for mortality; the protective association of BMI with mortality was confined to subgroups with high LV-GLS (>10.1%) or elderly patients (≥75 years). In men, this association was found in all subgroups without significant interaction. Metabolically healthy obese patients had better survival than metabolically unhealthy obese patients (log-rank p<0.001).
Conclusions: In women, a significant interaction was observed between BMI and age or LV-GLS in association with mortality, suggesting that sex, ageing and myocardial dysfunction can affect the magnitude of the obesity paradox in HF. Metabolic health status provides prognostic information beyond obesity status.
Trial registration number: Registry: ClinicalTrials.gov Number: NCT03513653 (https://clinicaltrials.gov/ct2/show/NCT03513653).
Keywords: Heart failure; left ventricular geometry; metabolic health status; myocardial function; obesity paradox; sex-related difference.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Left ventricular global longitudinal strain in patients with heart failure with preserved ejection fraction: outcomes following an acute heart failure hospitalization.ESC Heart Fail. 2017 Nov;4(4):432-439. doi: 10.1002/ehf2.12159. Epub 2017 Apr 20. ESC Heart Fail. 2017. PMID: 29154416 Free PMC article.
-
Subclinical alterations in left ventricular structure and function according to obesity and metabolic health status.PLoS One. 2019 Sep 12;14(9):e0222118. doi: 10.1371/journal.pone.0222118. eCollection 2019. PLoS One. 2019. PMID: 31513625 Free PMC article.
-
Relationship Between Myocardial Function, Body Mass Index, and Outcome After ST-Segment-Elevation Myocardial Infarction.Circ Cardiovasc Imaging. 2017 Jul;10(7):e005670. doi: 10.1161/CIRCIMAGING.116.005670. Circ Cardiovasc Imaging. 2017. PMID: 28701527
-
Complex interaction of obesity, intentional weight loss and heart failure: a systematic review and meta-analysis.Heart. 2020 Jan;106(1):58-68. doi: 10.1136/heartjnl-2019-314770. Epub 2019 Sep 17. Heart. 2020. PMID: 31530572
-
Anatomy of the obesity paradox in heart failure.Heart Fail Rev. 2014 Sep;19(5):621-35. doi: 10.1007/s10741-013-9406-7. Heart Fail Rev. 2014. PMID: 24037386 Review.
Cited by
-
Effect of obesity on cardiovascular responses to submaximal treadmill exercise in adult males.J Family Med Prim Care. 2020 Sep 30;9(9):4673-4679. doi: 10.4103/jfmpc.jfmpc_543_20. eCollection 2020 Sep. J Family Med Prim Care. 2020. PMID: 33209782 Free PMC article.
-
The Relationship Between Body Mass Index and In-hospital Survival in Patients Admitted With Acute Heart Failure.Front Cardiovasc Med. 2022 Apr 28;9:855525. doi: 10.3389/fcvm.2022.855525. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 35571201 Free PMC article.
-
Waist circumference is associated with major adverse cardiovascular events in male but not female patients with type-2 diabetes mellitus.Cardiovasc Diabetol. 2020 Mar 25;19(1):39. doi: 10.1186/s12933-020-01007-6. Cardiovasc Diabetol. 2020. PMID: 32213183 Free PMC article.
-
Abdominal Obesity Is Associated with an Increased Risk of All-Cause Mortality in Males but Not in Females with HFpEF.Cardiovasc Ther. 2022 Apr 9;2022:2950055. doi: 10.1155/2022/2950055. eCollection 2022. Cardiovasc Ther. 2022. PMID: 35586579 Free PMC article.
-
Obesity: the perfect storm for heart failure.ESC Heart Fail. 2024 Aug;11(4):1841-1860. doi: 10.1002/ehf2.14641. Epub 2024 Mar 15. ESC Heart Fail. 2024. PMID: 38491741 Free PMC article. Review.
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous