

First-in-human robotic supermicrosurgery using a dedicated microsurgical robot for treating breast cancer-related lymphedema: a randomized pilot trial
- PMID: 32047155
- PMCID: PMC7012819
- DOI: 10.1038/s41467-019-14188-w
First-in-human robotic supermicrosurgery using a dedicated microsurgical robot for treating breast cancer-related lymphedema: a randomized pilot trial
Abstract
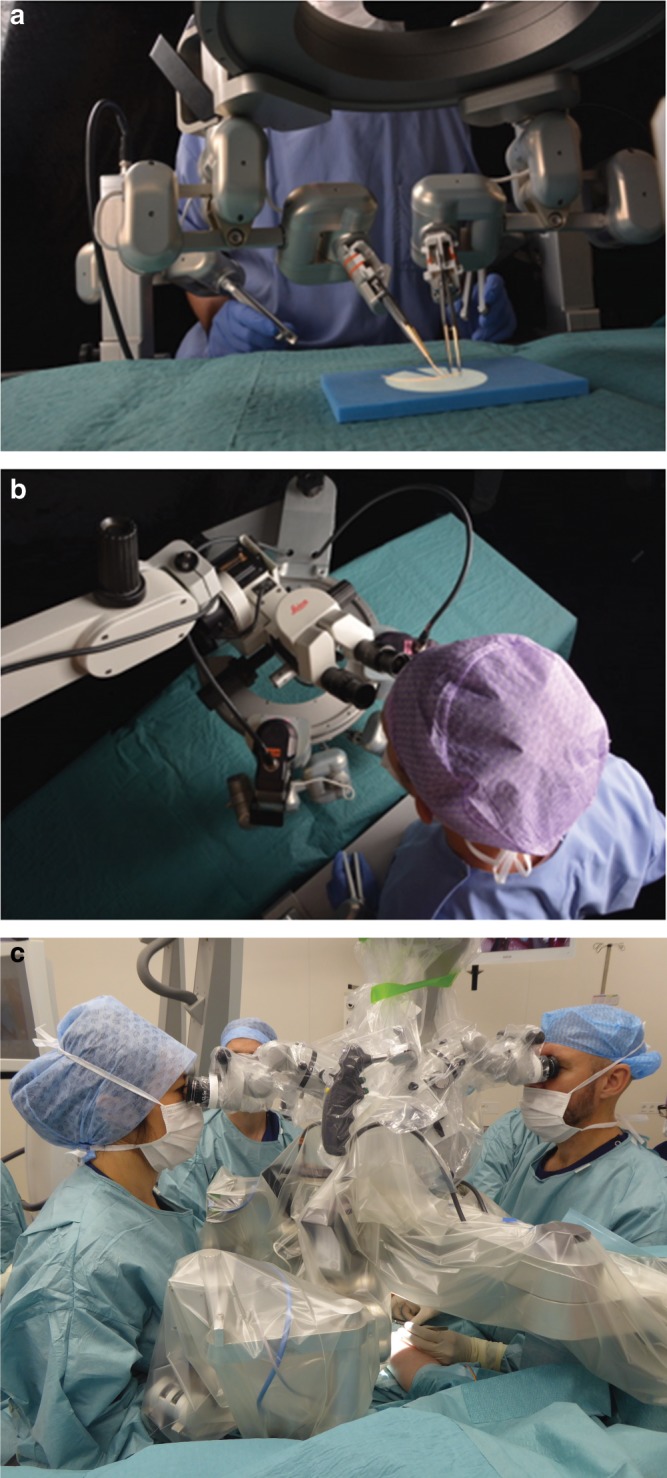
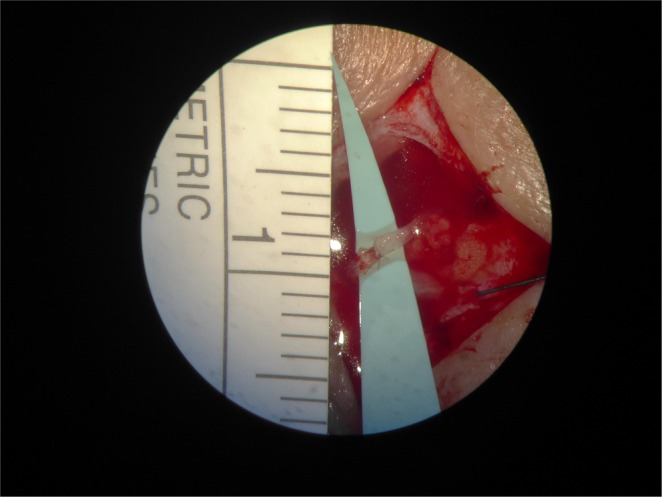
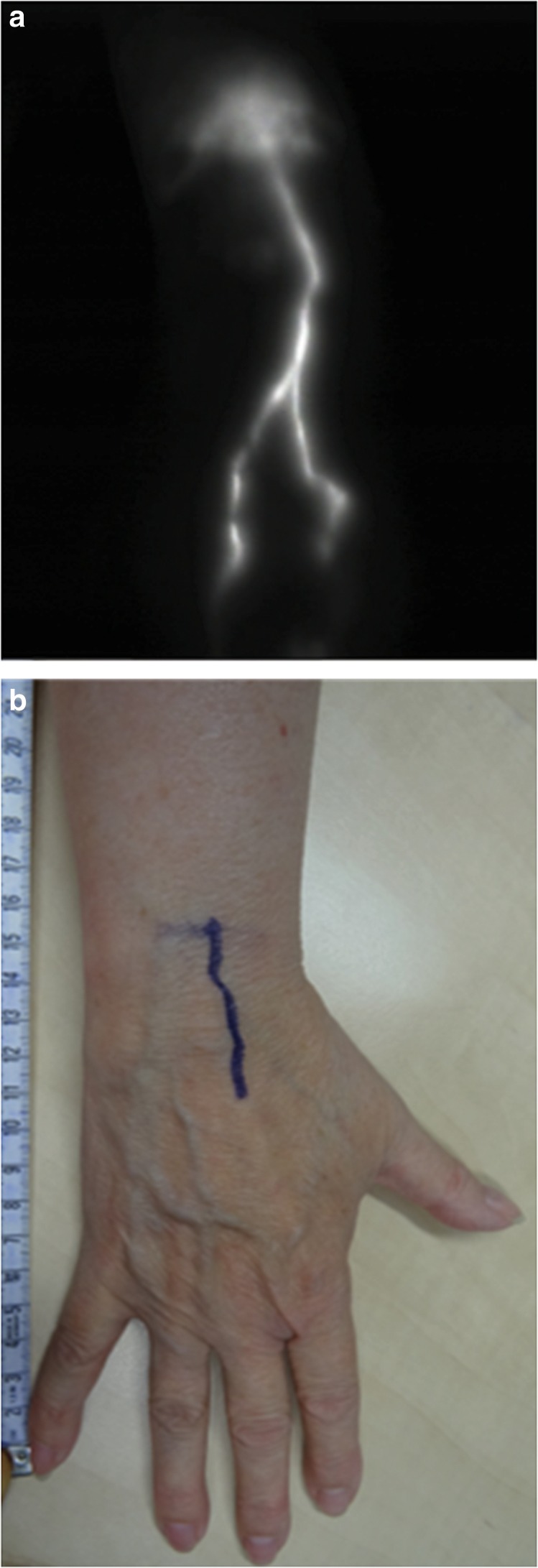
Advancements in reconstructive microsurgery have evolved into supermicrosurgery; connecting vessels with diameter between 0.3 and 0.8 mm for reconstruction of lymphatic flow and vascularized tissue transplantation. Supermicrosurgery is limited by the precision and dexterity of the surgeon's hands. Robot assistance can help overcome these human limitations, thereby enabling a breakthrough in supermicrosurgery. We report the first-in-human study of robot-assisted supermicrosurgery using a dedicated microsurgical robotic platform. A prospective randomized pilot study is conducted comparing robot-assisted and manual supermicrosurgical lymphatico-venous anastomosis (LVA) in treating breast cancer-related lymphedema. We evaluate patient outcome at 1 and 3 months post surgery, duration of the surgery, and quality of the anastomosis. At 3 months, patient outcome improves. Furthermore, a steep decline in duration of time required to complete the anastomosis is observed in the robot-assisted group (33-16 min). Here, we report the feasibility of robot-assisted supermicrosurgical anastomosis in LVA, indicating promising results for the future of reconstructive supermicrosurgery.
Conflict of interest statement
The authors declare the following competing interests: R.M.S., A.M.J.S., B.W., F.S., S.S.Q. MicroSurgical Robot research group—no relevant conflict of interest. T.J.M.v.M., chief medical officer at MicroSure (shareholder). R.R.W.J.v.d.H., shareholder in MicroSure. R.C., chief technical officer at MicroSure (shareholder).
Figures
Comment in
-
Robot-assisted supermicrosurgery for lymphoedema.Lancet Oncol. 2020 Mar;21(3):e134. doi: 10.1016/S1470-2045(20)30102-9. Epub 2020 Feb 20. Lancet Oncol. 2020. PMID: 32087769 No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
