

Remote Ischaemic Preconditioning Reduces Kidney Injury Biomarkers in Patients Undergoing Open Surgical Lower Limb Revascularisation: A Randomised Trial
- PMID: 32047578
- PMCID: PMC7003258
- DOI: 10.1155/2020/7098505
Remote Ischaemic Preconditioning Reduces Kidney Injury Biomarkers in Patients Undergoing Open Surgical Lower Limb Revascularisation: A Randomised Trial
Abstract
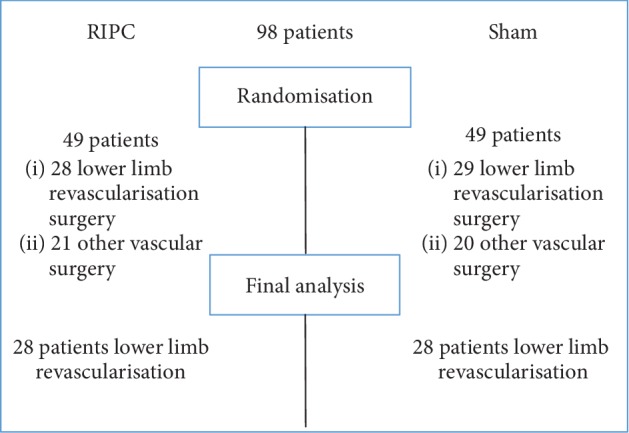
Background and aims: Perioperative kidney injury affects 12.7% of patients undergoing lower limb revascularisation surgery. Remote ischaemic preconditioning (RIPC) is a potentially protective procedure against organ damage and consists of short nonlethal episodes of ischaemia. The main objective of this substudy was to evaluate the effect of RIPC on kidney function, inflammation, and oxidative stress in patients undergoing open surgical lower limb revascularisation. Materials and Methods. This is a subgroup analysis of a randomised, sham-controlled, double-blinded, single-centre study. A RIPC or a sham procedure was performed noninvasively along with preparation for anaesthesia in patients undergoing open surgical lower limb revascularisation. The RIPC protocol consisted of 4 cycles of 5 minutes of ischaemia, with 5 minutes of reperfusion between every episode. Blood was collected for analysis preoperatively, 2, 8, and 24 hours after surgery, and urine was collected preoperatively and 24 hours after surgery.
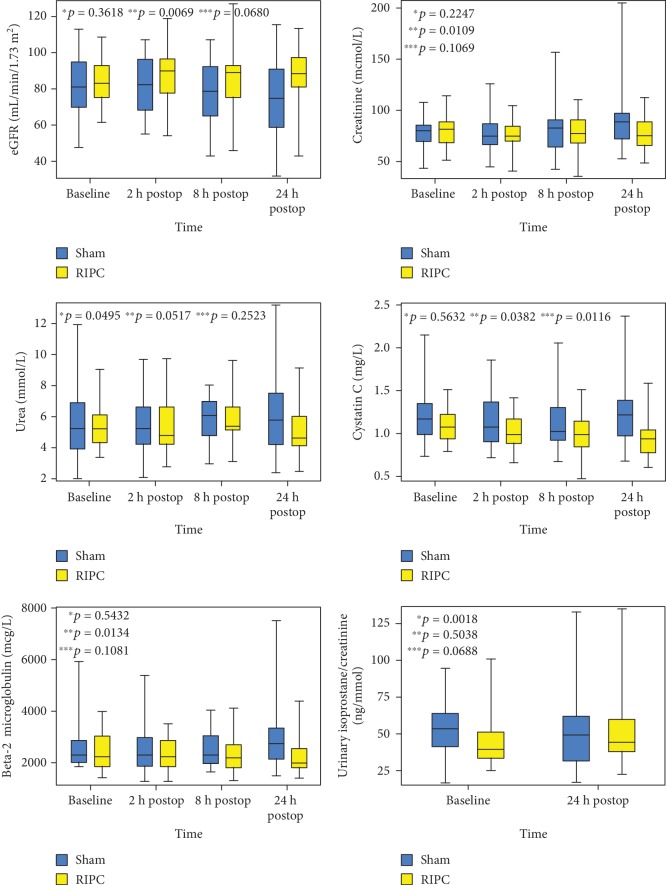
Results: Data of 56 patients were included in the analysis. Serum creatinine, cystatin C, and beta-2 microglobulin increased, and eGFR decreased across all time points significantly more in the sham group than in the RIPC group (p = 0.021, p = 0.021, p = 0.021, p = 0.021, p = 0.021.
Conclusions: Our finding of reduced release of kidney injury biomarkers may indicate the renoprotective effect of RIPC in patients undergoing open surgical lower limb revascularisation. The trial is registered with ClinicalTrials.gov NCT02689414.
Copyright © 2020 Teele Kasepalu et al.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures
Similar articles
-
The Effect of Remote Ischaemic Preconditioning on Arterial Stiffness in Patients Undergoing Vascular Surgery: A Randomised Clinical Trial.Eur J Vasc Endovasc Surg. 2019 Jun;57(6):868-875. doi: 10.1016/j.ejvs.2018.12.002. Epub 2019 May 22. Eur J Vasc Endovasc Surg. 2019. PMID: 31126835 Clinical Trial.
-
Remote Ischaemic Preconditioning Attenuates Cardiac Biomarkers During Vascular Surgery: A Randomised Clinical Trial.Eur J Vasc Endovasc Surg. 2020 Feb;59(2):301-308. doi: 10.1016/j.ejvs.2019.09.502. Epub 2019 Dec 20. Eur J Vasc Endovasc Surg. 2020. PMID: 31870692 Clinical Trial.
-
Effect of remote ischaemic preconditioning on renal protection in patients undergoing laparoscopic partial nephrectomy: a 'blinded' randomised controlled trial.BJU Int. 2013 Jul;112(1):74-80. doi: 10.1111/bju.12004. Epub 2013 Mar 4. BJU Int. 2013. PMID: 23452148 Clinical Trial.
-
Effect of Remote Ischaemic preconditioning on Clinical outcomes in patients undergoing Coronary Artery bypass graft surgery (ERICCA study): a multicentre double-blind randomised controlled clinical trial.Southampton (UK): NIHR Journals Library; 2016 Jun. Southampton (UK): NIHR Journals Library; 2016 Jun. PMID: 27359023 Free Books & Documents. Review.
-
Remote ischemic preconditioning for prevention of acute kidney injury: a meta-analysis of randomized controlled trials.Am J Kidney Dis. 2014 Oct;64(4):574-83. doi: 10.1053/j.ajkd.2014.04.029. Epub 2014 Jun 20. Am J Kidney Dis. 2014. PMID: 24954246
Cited by
-
The Role of RIPC in Preventing Organ Damage, Inflammation, and Oxidative Stress during Lower Limb DSA: A Randomised Controlled Trial.Oxid Med Cell Longev. 2021 Dec 8;2021:6043550. doi: 10.1155/2021/6043550. eCollection 2021. Oxid Med Cell Longev. 2021. PMID: 34925697 Free PMC article. Clinical Trial.
-
Tourniquet-induced lower limb ischemia/reperfusion reduces mitochondrial function by decreasing mitochondrial biogenesis in acute kidney injury in mice.Physiol Rep. 2022 Feb;10(3):e15181. doi: 10.14814/phy2.15181. Physiol Rep. 2022. PMID: 35146957 Free PMC article.
-
Remote ischaemic preconditioning for transcatheter aortic valve replacement: a protocol for a systematic review with meta-analysis and trial sequential analysis.BMJ Open. 2024 Apr 25;14(4):e080200. doi: 10.1136/bmjopen-2023-080200. BMJ Open. 2024. PMID: 38670623 Free PMC article.
-
Remote ischaemic preconditioning versus no remote ischaemic preconditioning for vascular and endovascular surgical procedures.Cochrane Database Syst Rev. 2023 Jan 16;1(1):CD008472. doi: 10.1002/14651858.CD008472.pub3. Cochrane Database Syst Rev. 2023. PMID: 36645250 Free PMC article.
-
Remote ischaemic preconditioning in cemented hip arthroplasty (the PRINCIPAL study)-randomised controlled trial: study protocol.BMJ Open. 2025 Jun 23;15(6):e096433. doi: 10.1136/bmjopen-2024-096433. BMJ Open. 2025. PMID: 40550717 Free PMC article.
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
