

The pathology of central nervous system inflammatory demyelinating disease accompanying myelin oligodendrocyte glycoprotein autoantibody
- PMID: 32048003
- PMCID: PMC7181560
- DOI: 10.1007/s00401-020-02132-y
The pathology of central nervous system inflammatory demyelinating disease accompanying myelin oligodendrocyte glycoprotein autoantibody
Abstract
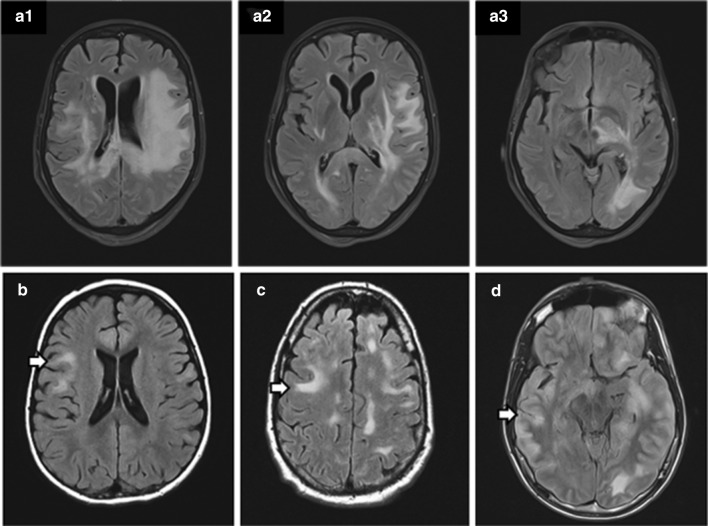
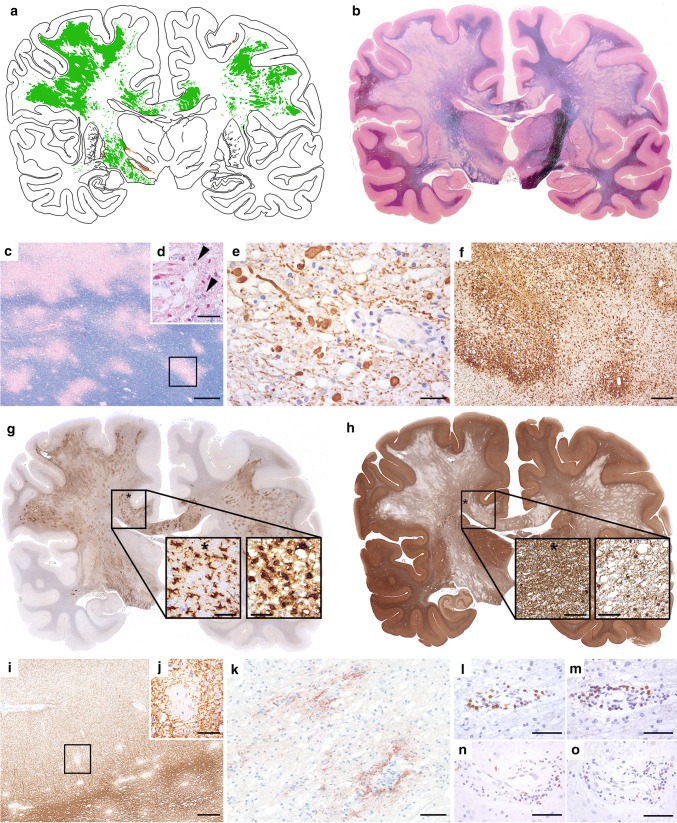
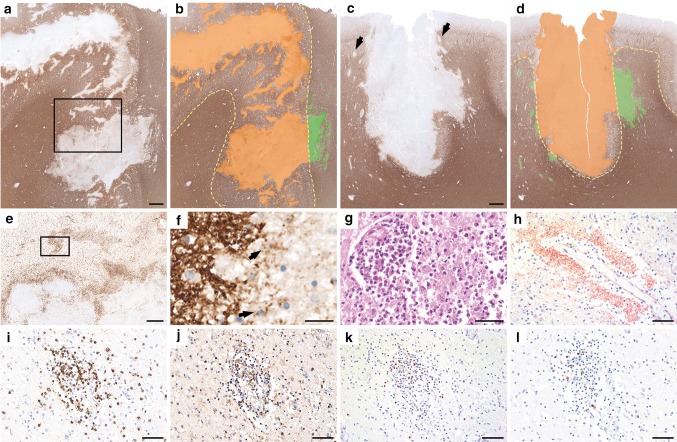
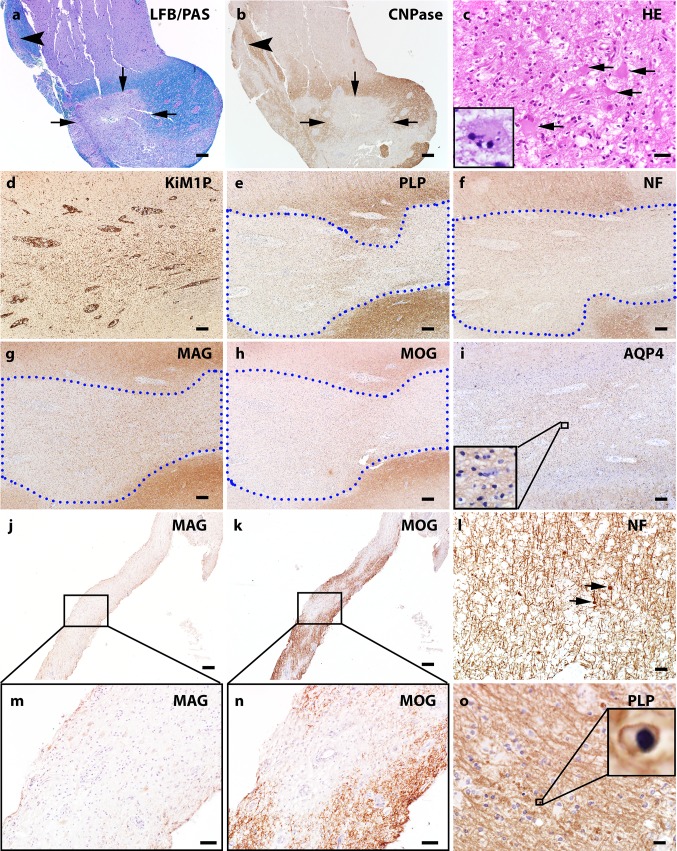
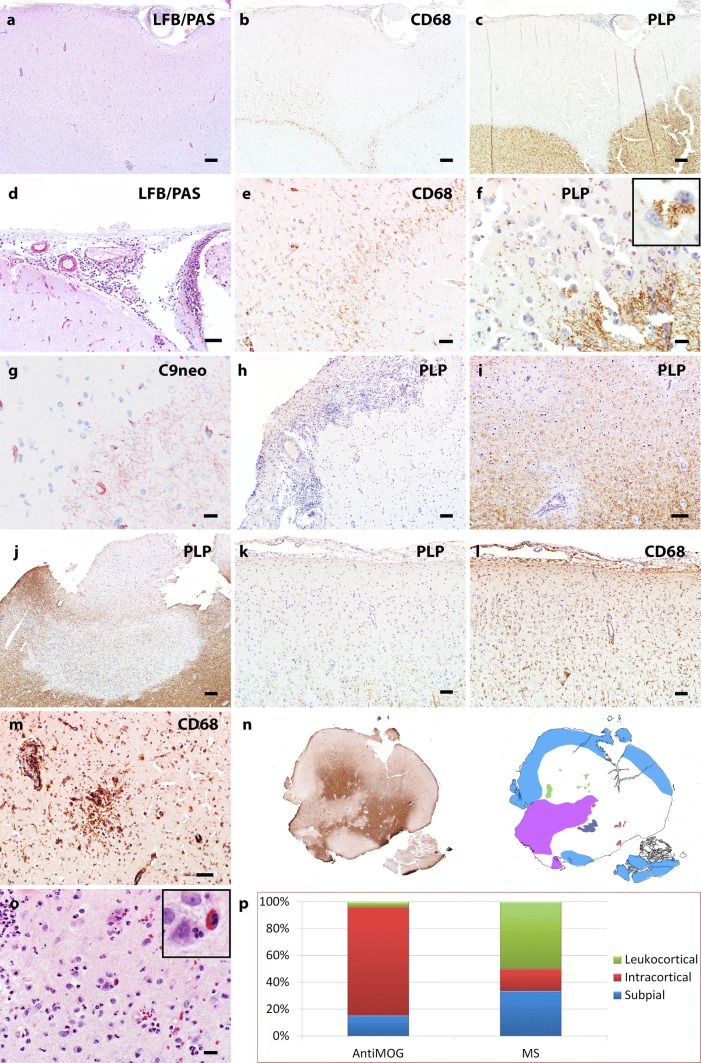
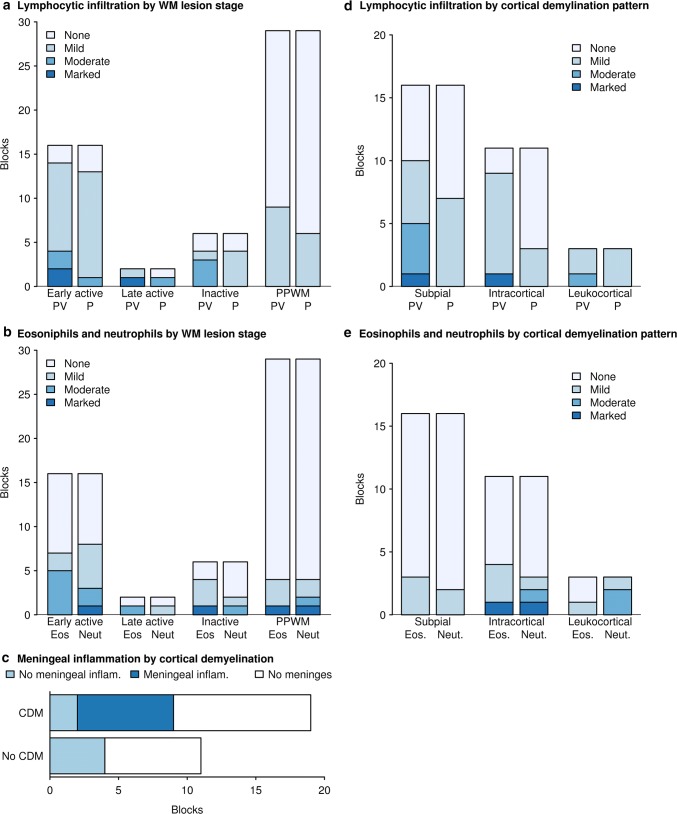
We sought to define the pathological features of myelin oligodendrocyte glycoprotein (MOG) antibody associated disorders (MOGAD) in an archival autopsy/biopsy cohort. We histopathologically analyzed 2 autopsies and 22 brain biopsies from patients with CNS inflammatory demyelinating diseases seropositive for MOG-antibody by live-cell-based-assay with full length MOG in its conformational form. MOGAD autopsies (ages 52 and 67) demonstrate the full spectrum of histopathological features observed within the 22 brain biopsies (median age, 10 years; range, 1-66; 56% female). Clinical, radiologic, and laboratory characteristics and course (78% relapsing) are consistent with MOGAD. MOGAD pathology is dominated by coexistence of both perivenous and confluent white matter demyelination, with an over-representation of intracortical demyelinated lesions compared to typical MS. Radially expanding confluent slowly expanding smoldering lesions in the white matter as seen in MS, are not present. A CD4+ T-cell dominated inflammatory reaction with granulocytic infiltration predominates. Complement deposition is present in all active white matter lesions, but a preferential loss of MOG is not observed. AQP4 is preserved, with absence of dystrophic astrocytes, and variable oligodendrocyte and axonal destruction. MOGAD is pathologically distinguished from AQP4-IgG seropositive NMOSD, but shares some overlapping features with both MS and ADEM, suggesting a transitional pathology. Complement deposition in the absence of selective MOG protein loss suggest humoral mechanisms are involved, however argue against endocytic internalization of the MOG antigen. Parallels with MOG-EAE suggest MOG may be an amplification factor that augments CNS demyelination, possibly via complement mediated destruction of myelin or ADCC phagocytosis.
Keywords: Acute disseminated encephalomyelitis; Autopsy; Biopsy; Demyelination; MOG; Multiple sclerosis.
Conflict of interest statement
No authors had conflicts of interests relevant to this study.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
