

Development of the human heart
- PMID: 32048790
- PMCID: PMC7078965
- DOI: 10.1002/ajmg.c.31778
Development of the human heart
Abstract
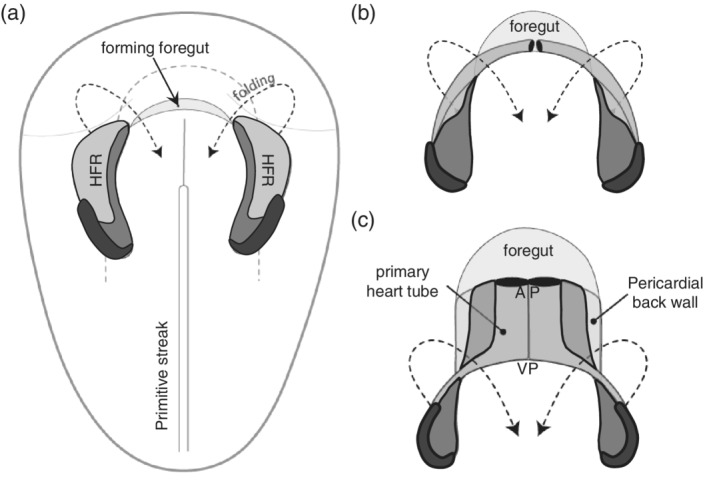
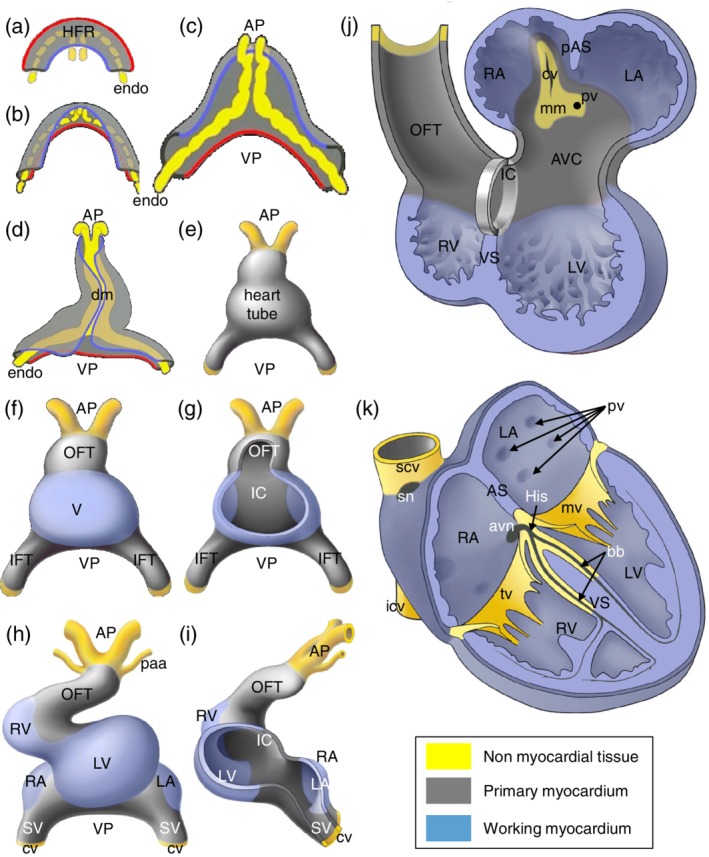
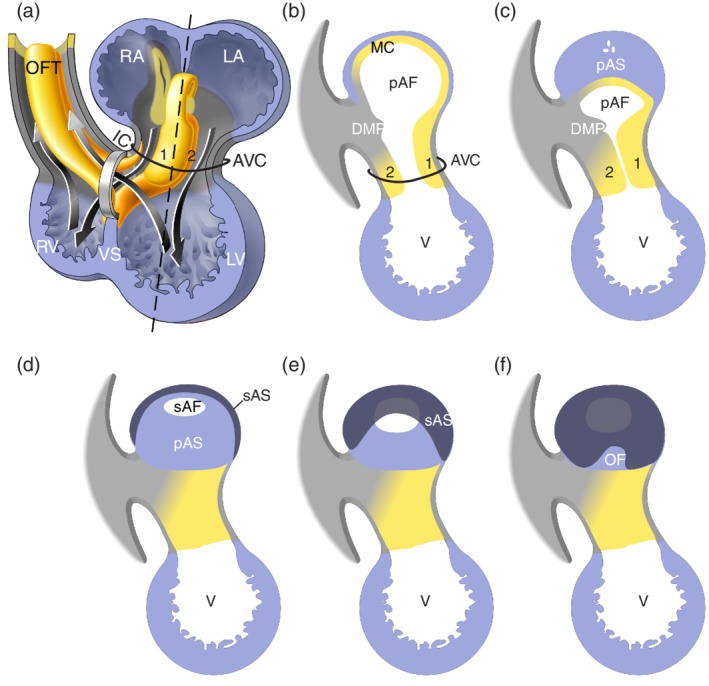
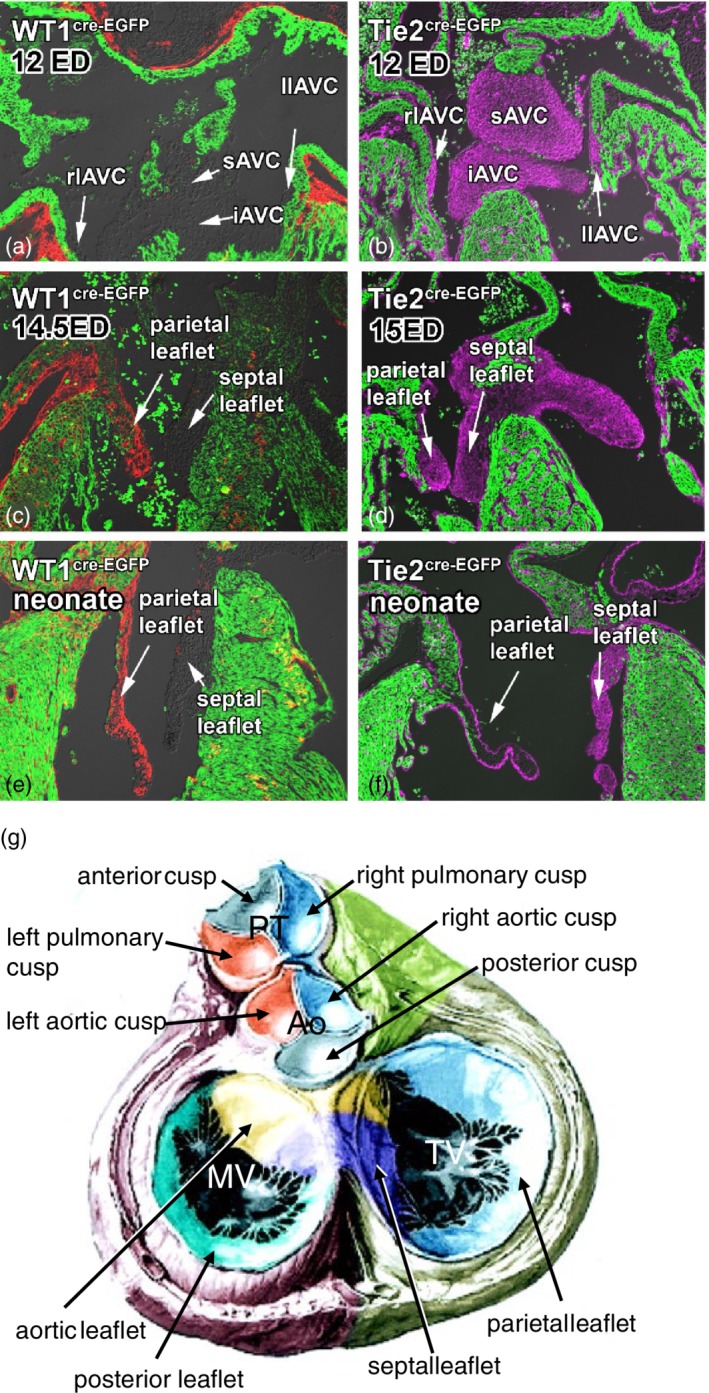
In 2014, an extensive review discussing the major steps of cardiac development focusing on growth, formation of primary and chamber myocardium and the development of the cardiac electrical system, was published. Molecular genetic lineage analyses have since furthered our insight in the developmental origin of the various component parts of the heart, which currently can be unambiguously identified by their unique molecular phenotype. Moreover, genetic, molecular and cell biological analyses have driven insights into the mechanisms underlying the development of the different cardiac components. Here, we build on our previous review and provide an insight into the molecular mechanistic revelations that have forwarded the field of cardiac development. Despite the enormous advances in our knowledge over the last decade, the development of congenital cardiac malformations remains poorly understood. The challenge for the next decade will be to evaluate the different developmental processes using newly developed molecular genetic techniques to further unveil the gene regulatory networks operational during normal and abnormal cardiac development.
Keywords: cardiac development; cardiac growth; epicardial development; septation; valve development.
© 2020 The Authors. American Journal of Medical Genetics Part C: Seminars in Medical Genetics published by Wiley Periodicals, Inc.
Figures
References
-
- Aanhaanen, W. T. , Boukens, B. J. , Sizarov, A. , Wakker, V. , de Gier‐de Vries, C. , van Ginneken, A. C. , … Christoffels, V. M. (2011). Defective Tbx2‐dependent patterning of the atrioventricular canal myocardium causes accessory pathway formation in mice. Journal of Clinical Investigation, 121(2), 534–544. - PMC - PubMed
-
- Aanhaanen, W. T. , Mommersteeg, M. T. , Norden, J. , Wakker, V. , de Gier‐de Vries, C. , Anderson, R. H. , … Christoffels, V. M. (2010). Developmental origin, growth, and three‐dimensional architecture of the atrioventricular conduction axis of the mouse heart. Circulation Research, 107(6), 728–736. - PubMed
-
- Anderson, R. H. , Brown, N. A. , Webb, S. , Chaudhry, B. , Henderson, D. , & Moorman, A. F. M. (2009). In Mikhailov A.T. & Torrado M. (Eds.). Morphology of the developing cardiac outflow tract. Transworld Research Network.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
