

Impact of myocardial fibrosis on left ventricular remodelling, recovery, and outcome after transcatheter aortic valve implantation in different haemodynamic subtypes of severe aortic stenosis
- PMID: 32049275
- PMCID: PMC7242071
- DOI: 10.1093/eurheartj/ehaa033
Impact of myocardial fibrosis on left ventricular remodelling, recovery, and outcome after transcatheter aortic valve implantation in different haemodynamic subtypes of severe aortic stenosis
Abstract
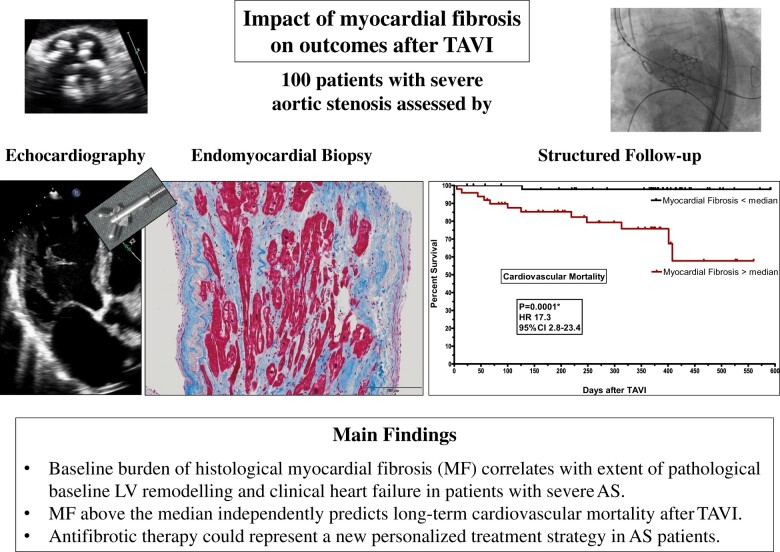
Aims: Myocardial fibrosis (MF) might represent a key player in pathophysiology of heart failure in aortic stenosis (AS). We aimed to assess its impact on left ventricular (LV) remodelling, recovery, and mortality after transcatheter aortic valve implantation (TAVI) in different AS subtypes.
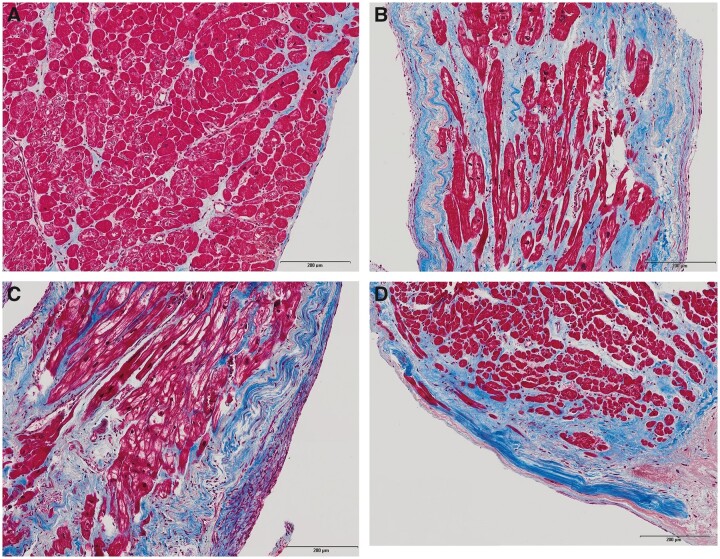
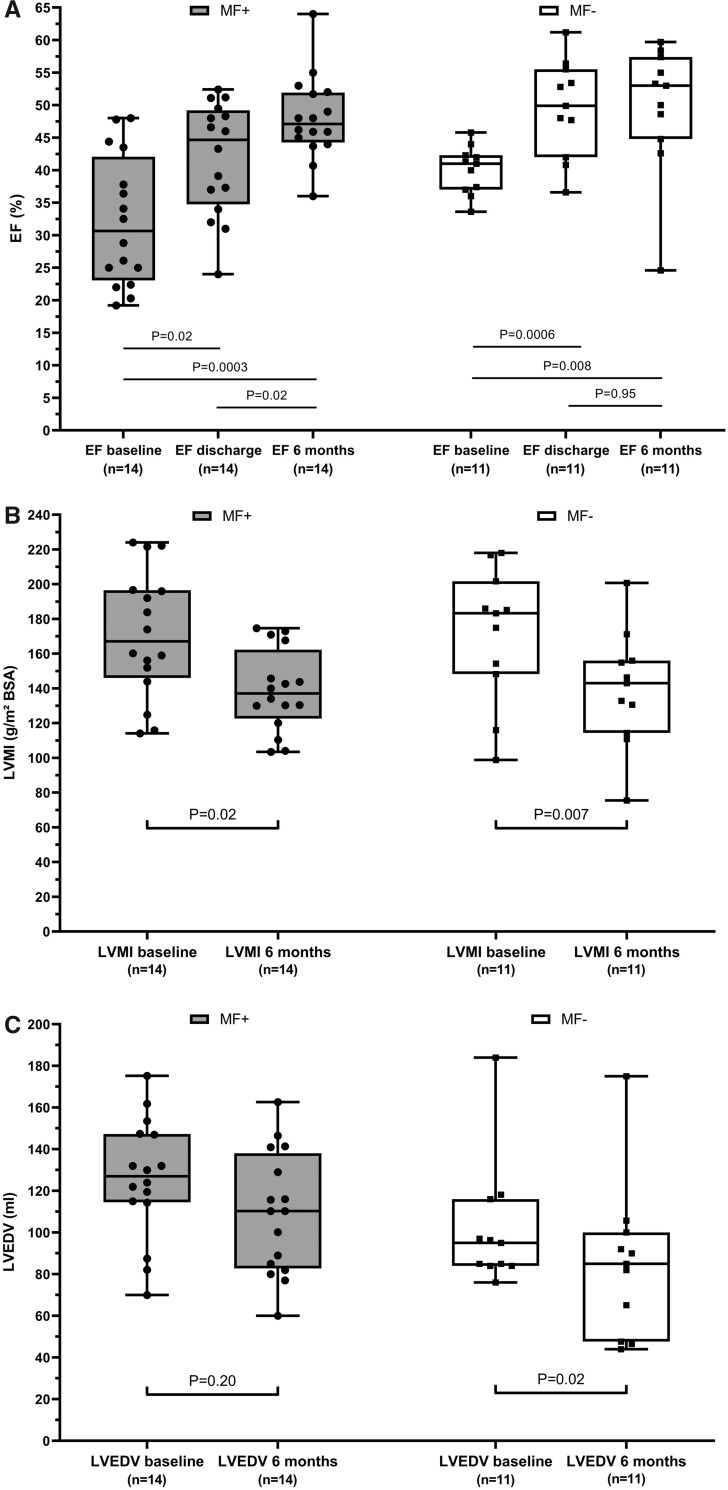
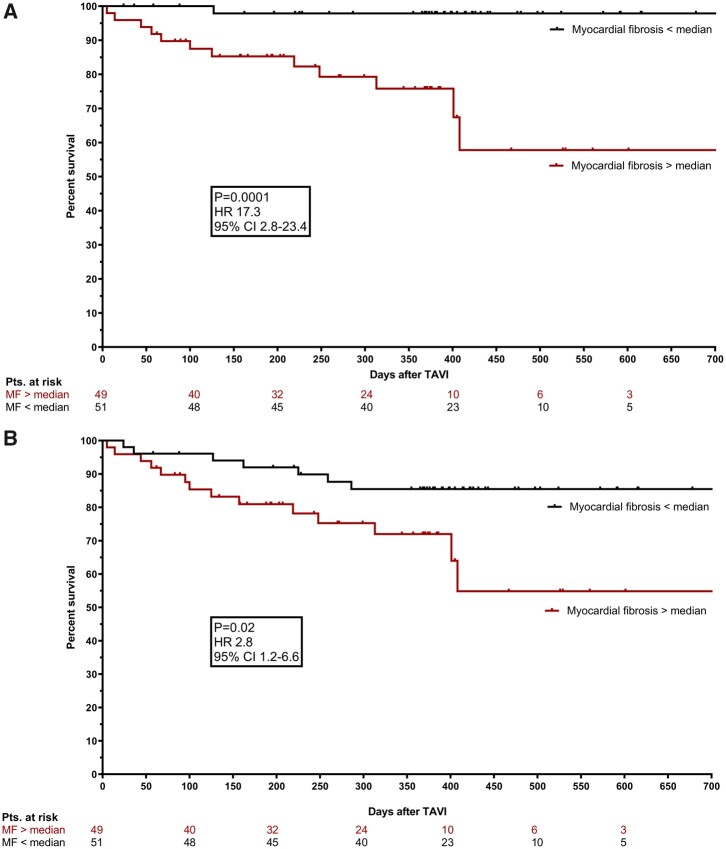
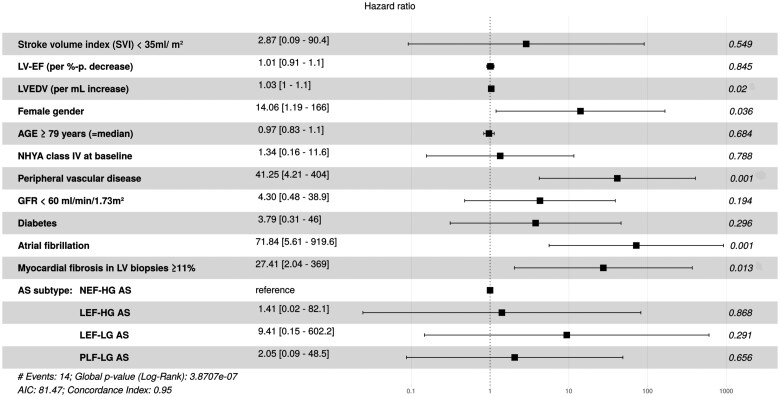
Methods and results: One hundred patients with severe AS were prospectively characterized clinically and echocardiographically at baseline (BL), 6 months, 1 year, and 2 years following TAVI. Left ventricular biopsies were harvested after valve deployment. Myocardial fibrosis was assessed after Masson's trichrome staining, and fibrotic area was calculated as percentage of total tissue area. Patients were stratified according to MF above (MF+) or below (MF-) median percentage MF (≥11% or <11%). Myocardial fibrosis burden differed significantly between AS subtypes, with highest levels in low ejection fraction (EF), low-gradient AS and lowest levels in normal EF, high-gradient AS (29.5 ± 26.4% vs. 13.5 ± 16.1%, P = 0.003). In the entire cohort, MF+ was significantly associated with poorer LV function, higher extent of pathological LV remodelling, and more pronounced clinical heart failure at BL. After TAVI, MF+ was associated with a delay in normalization of LV geometry and function but not per se with absence of reverse remodelling and clinical improvement. However, 22 patients died during follow-up (mean, 11 months), and 14 deaths were classified as cardiovascular (CV) (n = 9 arrhythmia-associated). Importantly, 13 of 14 CV deaths occurred in MF+ patients (CV mortality 26.5% in MF+ vs. 2% in MF- patients, P = 0.0003). Multivariate analysis identified MF+ as independent predictor of CV mortality [hazard ratio (HR) 27.4 (2.0-369), P = 0.01].
Conclusion: Histological MF is associated with AS-related pathological LV remodelling and independently predicts CV mortality after TAVI.
Keywords: Aortic stenosis; Endomyocardial biopsy; Myocardial fibrosis; Transcatheter aortic valve implantation.
© The Author(s) 2020. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures

Comment in
-
Left ventricular myocardial fibrosis: a marker of bad prognosis in symptomatic severe aortic stenosis.Eur Heart J. 2020 May 21;41(20):1915-1917. doi: 10.1093/eurheartj/ehaa151. Eur Heart J. 2020. PMID: 32211751 No abstract available.
References
-
- Baumgartner H, Falk V, Bax JJ, De Bonis M, Hamm C, Holm PJ, Iung B, Lancellotti P, Lansac E, Rodriguez Muñoz D, Rosenhek R, Sjögren J, Tornos Mas P, Vahanian A, Walther T, Wendler O, Windecker S, Zamorano JL; ESC Scientific Document Group. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J 2017;38:2739–2791. - PubMed
-
- Hein S, Arnon E, Kostin S, SchöNburg M, ElsäSser A, Polyakova V, Bauer EP, KlöVekorn W-P, Schaper J. Progression from compensated hypertrophy to failure in the pressure-overloaded human heart: structural deterioration and compensatory mechanisms. Circulation 2003;107:984–991. - PubMed
-
- Krayenbuehl HP, Hess OM, Monrad ES, Schneider J, Mall G, Turina M. Left ventricular myocardial structure in aortic valve disease before, intermediate, and late after aortic valve replacement. Circulation 1989;79:744–755. - PubMed
-
- Weidemann F, Herrmann S, StöRk S, Niemann M, Frantz S, Lange V, Beer M, GattenlöHner S, Voelker W, Ertl G, Strotmann JrgM. Impact of myocardial fibrosis in patients with symptomatic severe aortic stenosis. Circulation 2009;120:577–584. - PubMed
-
- Azevedo CF, Nigri M, Higuchi ML, Pomerantzeff PM, Spina GS, Sampaio RO, Tarasoutchi F, Grinberg M, Rochitte CE. Prognostic significance of myocardial fibrosis quantification by histopathology and magnetic resonance imaging in patients with severe aortic valve disease. J Am Coll Cardiol 2010;56:278–287. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
