

Association of Monogenic vs Polygenic Hypercholesterolemia With Risk of Atherosclerotic Cardiovascular Disease
- PMID: 32049305
- PMCID: PMC7042820
- DOI: 10.1001/jamacardio.2019.5954
Association of Monogenic vs Polygenic Hypercholesterolemia With Risk of Atherosclerotic Cardiovascular Disease
Erratum in
-
Error in Figure 3.JAMA Cardiol. 2020 Apr 1;5(4):488. doi: 10.1001/jamacardio.2020.0459. JAMA Cardiol. 2020. PMID: 32159730 Free PMC article. No abstract available.
Abstract
Importance: Monogenic familial hypercholesterolemia (FH) is associated with lifelong elevations in low-density lipoprotein cholesterol (LDL-C) levels and increased risk of atherosclerotic cardiovascular disease (CVD). However, many individuals with hypercholesterolemia have a polygenic rather than a monogenic cause for their condition. It is unclear if a genetic variant for hypercholesterolemia alters the risk of CVD.
Objectives: To assess whether a genetic variant for hypercholesterolemia alters the risk of atherosclerotic CVD and to evaluate how this risk compares with that of nongenetic hypercholesterolemia.
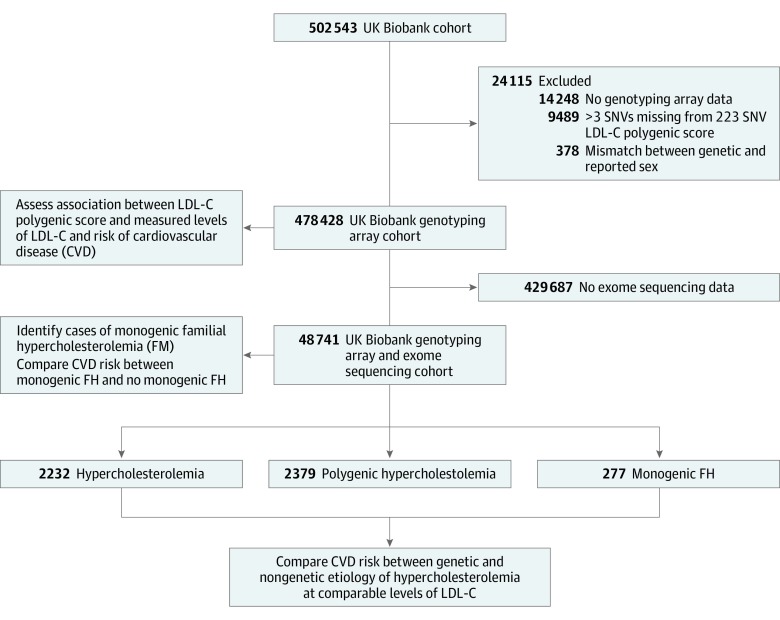
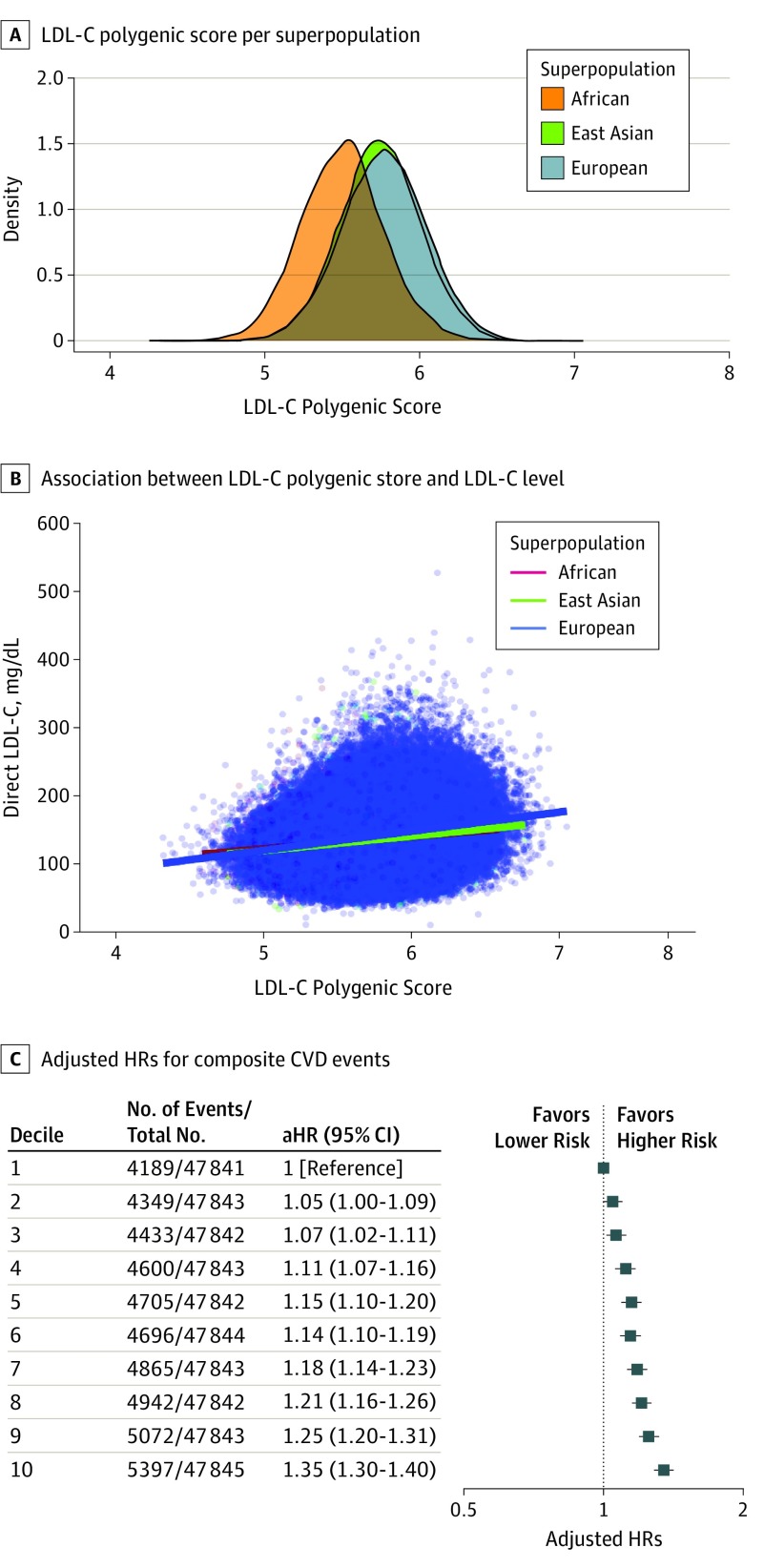
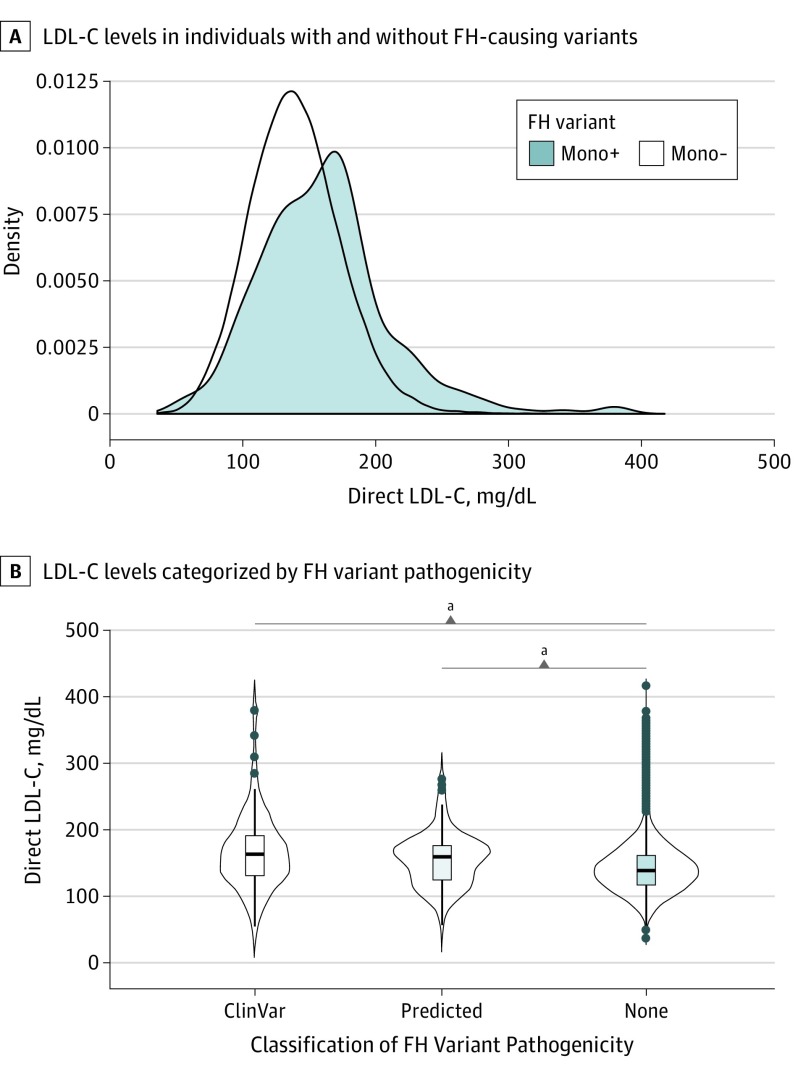
Design, setting, and participants: In this genetic-association, case-control, cohort study, individuals aged 40 to 69 years were recruited by the UK Biobank from across the United Kingdom between March 13, 2006, and October 1, 2010, and followed up until March 31, 2017. Genotyping array and exome sequencing data from the UK Biobank cohort were used to identify individuals with monogenic (LDLR, APOB, and PCSK9) or polygenic hypercholesterolemia (LDL-C polygenic score >95th percentile based on 223 single-nucleotide variants in the entire cohort). The data were analyzed from July 1, 2019, to December 30, 2019.
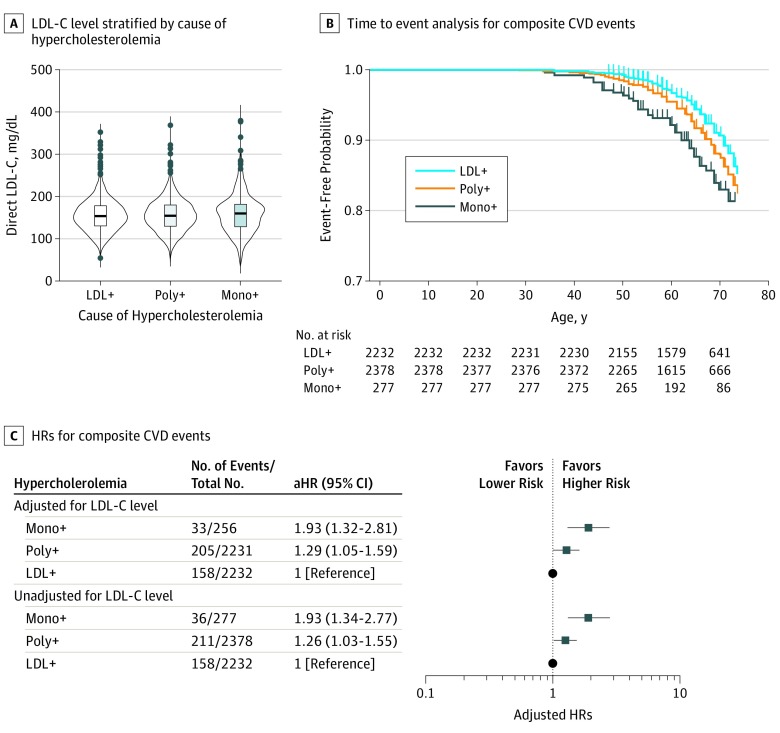
Main outcomes and measures: The study investigated the association of genotype with the risk of coronary and carotid revascularization, myocardial infarction, ischemic stroke, and all-cause mortality among the overall study population and among participants with monogenic FH (n = 277), polygenic hypercholesterolemia (n = 2379), or hypercholesterolemia with undetermined cause (n = 2232) at comparable levels of LDL-C measured at study enrollment.
Results: For the 48 741 individuals with genotyping array and exome sequencing data, the mean (SD) age was 56.6 (8.0) years, and 54.5% were female (n = 26 541 of 48 741). A monogenic FH variant for hypercholesterolemia was found in 277 individuals (0.57%, 1 in 176 individuals). Participants with monogenic FH were significantly more likely than those without monogenic FH to experience an atherosclerotic CVD event at 55 years or younger (17 of 277 [6.1%] vs 988 of 48 464 [2.0%]; P < .001). Compared with the general population, both monogenic and polygenic hypercholesterolemia were associated with an increased risk of CVD events. Moreover, among individuals with comparable levels of LDL-C, both monogenic (hazard ratio, 1.93; 95% CI, 1.34-2.77; P < .001) and polygenic hypercholesterolemia (hazard ratio, 1.26; 95% CI, 1.03-1.55; P = .03) were significantly associated with an increased risk of CVD events compared with the risk of such events in individuals with hypercholesterolemia without an identified genetic cause.
Conclusions and relevance: The findings of this study suggest that among individuals with hypercholesterolemia, genetic determinants of LDL-C levels may impose additional risk of CVD. Thus, understanding the possible genetic cause of hypercholesterolemia may provide important prognostic information to treat patients.
Conflict of interest statement
Figures
Comment in
-
Opportunities and Challenges for Polygenic Risk Scores in Prognostication and Prevention of Cardiovascular Disease.JAMA Cardiol. 2020 Apr 1;5(4):399-400. doi: 10.1001/jamacardio.2019.6232. JAMA Cardiol. 2020. PMID: 32049302 No abstract available.
-
Genetic Confirmation of Monogenic Familial Hypercholesterolemia Advises a More Intensive Lipid-Lowering Approach-Reply.JAMA Cardiol. 2020 Dec 1;5(12):1453. doi: 10.1001/jamacardio.2020.4120. JAMA Cardiol. 2020. PMID: 32936211 No abstract available.
-
Genetic Confirmation of Monogenic Familial Hypercholesterolemia Advises a More Intensive Lipid-Lowering Approach.JAMA Cardiol. 2020 Dec 1;5(12):1452-1453. doi: 10.1001/jamacardio.2020.4114. JAMA Cardiol. 2020. PMID: 32936217 No abstract available.
References
-
- Benn M, Watts GF, Tybjærg-Hansen A, Nordestgaard BG. Mutations causative of familial hypercholesterolaemia: screening of 98 098 individuals from the Copenhagen General Population Study estimated a prevalence of 1 in 217. Eur Heart J. 2016;37(17):1384-1394. doi: 10.1093/eurheartj/ehw028 - DOI - PubMed
-
- Ference BA, Ginsberg HN, Graham I, et al. Low-density lipoproteins cause atherosclerotic cardiovascular disease. 1. Evidence from genetic, epidemiologic, and clinical studies. A consensus statement from the European Atherosclerosis Society Consensus Panel. Eur Heart J. 2017;38(32):2459-2472. doi: 10.1093/eurheartj/ehx144 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
