

Comparison of the short-term outcomes between totally laparoscopic total gastrectomy and laparoscopic-assisted total gastrectomy for gastric cancer: a meta-analysis
- PMID: 32049863
- PMCID: PMC7035048
- DOI: 10.1097/MD.0000000000019225
Comparison of the short-term outcomes between totally laparoscopic total gastrectomy and laparoscopic-assisted total gastrectomy for gastric cancer: a meta-analysis
Abstract
Background: Totally laparoscopic total gastrectomy (TLTG) and laparoscopic-assisted total gastrectomy (LATG) are two common surgical approaches for upper and middle gastric cancer. Which surgical approach offers more advantages is still controversial due to a lack of evidence from randomized controlled trials (RCTs). This meta-analysis was conducted to compare the short-term outcomes between the two surgical approaches.
Methods: A systematic literature search was performed to evaluate short-term outcomes between TLTG and LATG, including overall postoperative complications, anastomosis-related complications, time for anastomosis, operation time, intraoperative blood loss, harvested lymph nodes, proximal margin, distal margin, time to first flatus, time to first diet, and postoperative hospital stay. Short-term outcomes were pooled and compared by meta-analysis using RevMan 5.3. Mean differences (MDs) or risk ratios (RRs) were calculated with 95% confidence intervals (CIs). P < .05 was considered statistically significant.
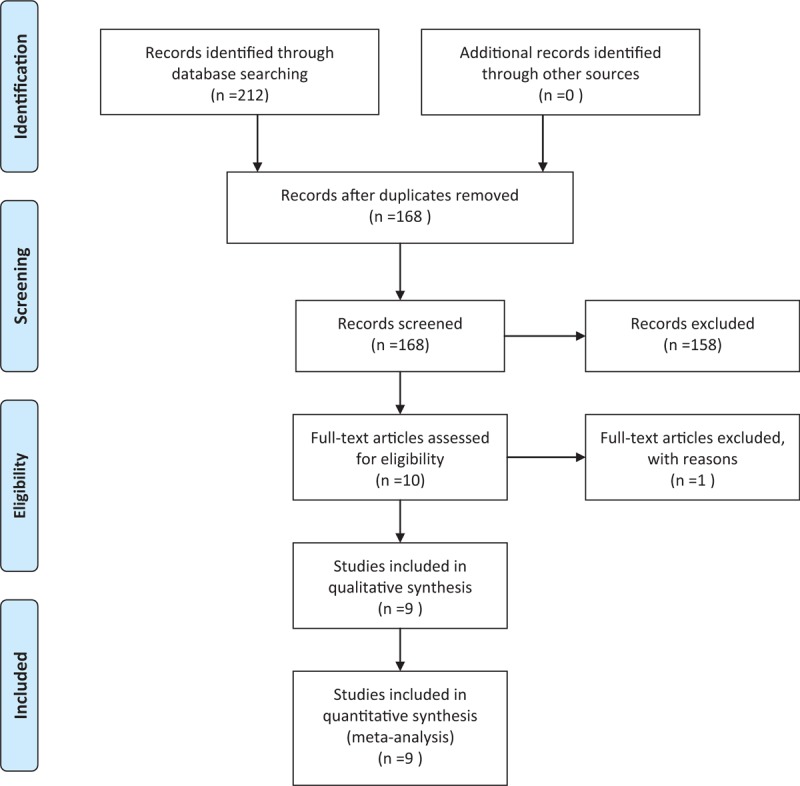
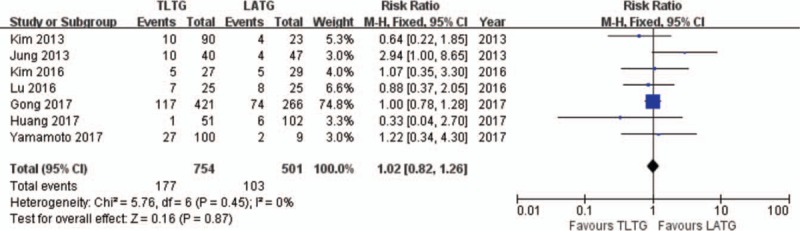
Results: A total of 9 cohort studies fulfilled the selection criteria. The total sample included 1671 cases. The meta-analysis showed no significant difference between the two surgical approaches in overall postoperative complications (RR = 1.02, 95% CI = 0.82 to 1.26, P = .87),anastomosis-related complications (RR = 0.64, 95%CI = 0.39 to 1.03, P = .06),time for anastomosis (MD = -5.13, 95% CI = -10.54 to 0.27, P = .06),operation time (MD = -10.68, 95% CI = -23.62 to 2.26, P = .11), intraoperative blood loss (MD = -25.58, 95% CI = -61.71 to 10.54, P = .17), harvested lymph nodes (MD = 1.61, 95% CI = -2.09 to 5.31, P = .39), proximal margin (MD = -0.37, 95% CI = -0.78 to 0.05, P = .09), distal margin (MD = 0.79, 95% CI = -0.57 to 2.14, P = .25), time to first flatus (MD = 0.01, 95% CI = -0.13 to 0.15, P = .87), time to first diet (MD = -0.22, 95% CI = -0.45 to 0.02, P = .07), and postoperative hospital stay (MD = -0.51, 95% CI = -1.10 to 0.07, P = .09).
Conclusions: TLTG is a safe and feasible surgical approach for upper and middle gastric cancer, with short-term outcomes that are similar to LATG. Nevertheless, high-quality, large-sample and multicenter RCTs are still required to further verify our conclusions.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
Similar articles
-
Comparison of totally laparoscopic total gastrectomy and laparoscopic-assisted total gastrectomy: A systematic review and meta-analysis.Int J Surg. 2019 Aug;68:1-10. doi: 10.1016/j.ijsu.2019.05.020. Epub 2019 Jun 9. Int J Surg. 2019. PMID: 31189084
-
Safety and effectiveness of totally laparoscopic total gastrectomy vs laparoscopic-assisted total gastrectomy: a meta-analysis.Int J Surg. 2024 Feb 1;110(2):1245-1265. doi: 10.1097/JS9.0000000000000921. Int J Surg. 2024. PMID: 38016295 Free PMC article.
-
Comparison efficacy and safety of total laparoscopic gastrectomy and laparoscopically assisted total gastrectomy in treatment of gastric cancer.World J Gastrointest Surg. 2024 Jun 27;16(6):1871-1882. doi: 10.4240/wjgs.v16.i6.1871. World J Gastrointest Surg. 2024. PMID: 38983345 Free PMC article.
-
Totally laparoscopic versus laparoscopic-assisted total gastrectomy for upper and middle gastric cancer: a single-unit experience of 253 cases with meta-analysis.World J Surg Oncol. 2016 Mar 31;14:96. doi: 10.1186/s12957-016-0860-2. World J Surg Oncol. 2016. PMID: 27036540 Free PMC article.
-
Efficacy of totally laparoscopic compared with laparoscopic-assisted total gastrectomy for gastric cancer: A meta-analysis.World J Clin Cases. 2020 Mar 6;8(5):900-911. doi: 10.12998/wjcc.v8.i5.900. World J Clin Cases. 2020. PMID: 32190626 Free PMC article.
Cited by
-
Development and validation of a LASSO-based nomogram for predicting anastomotic leakage in elderly patients after laparoscopic gastrectomy.J Gastrointest Oncol. 2025 Jun 30;16(3):922-936. doi: 10.21037/jgo-2024-897. Epub 2025 Jun 18. J Gastrointest Oncol. 2025. PMID: 40672095 Free PMC article.
-
[Evidence in minimally invasive oncological gastric surgery].Chirurg. 2021 Apr;92(4):304-315. doi: 10.1007/s00104-020-01315-3. Chirurg. 2021. PMID: 33245365 German.
-
Comparing intracorporeal mechanical anastomosis vs. hand-sewn esophagojejunostomy after total laparoscopic gastrectomy for esophagogastric junction cancer: a single-center study.World J Surg Oncol. 2023 Jan 17;21(1):12. doi: 10.1186/s12957-023-02889-y. World J Surg Oncol. 2023. PMID: 36650555 Free PMC article.
-
Comparison of short-term efficacy between totally laparoscopic gastrectomy and laparoscopic assisted gastrectomy for elderly patients with gastric cancer.World J Gastrointest Surg. 2022 Sep 27;14(9):950-962. doi: 10.4240/wjgs.v14.i9.950. World J Gastrointest Surg. 2022. PMID: 36185561 Free PMC article.
-
A case series of 10 patients undergone linear cutter/stapler guiding device-led overlapped esophagojejunostomy: a preliminary study.J Gastrointest Oncol. 2023 Apr 29;14(2):617-625. doi: 10.21037/jgo-23-193. J Gastrointest Oncol. 2023. PMID: 37201061 Free PMC article.
References
-
- Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer 2015;136:E359–86. - PubMed
-
- Torre LA, Bray F, Siegel RL, et al. Global cancer statistics, 2012. CA Cancer J Clin 2015;65:87–108. - PubMed
-
- Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2018;68:394–424. - PubMed
-
- Ajani JA, D’Amico TA, Almhanna K, et al. Gastric Cancer, Version 3.2016, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw 2016;14:1286–312. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
