

Long-term mortality and outcome in hospital survivors of septic shock, sepsis, and severe infections: The importance of aftercare
- PMID: 32050005
- PMCID: PMC7015408
- DOI: 10.1371/journal.pone.0228952
Long-term mortality and outcome in hospital survivors of septic shock, sepsis, and severe infections: The importance of aftercare
Abstract
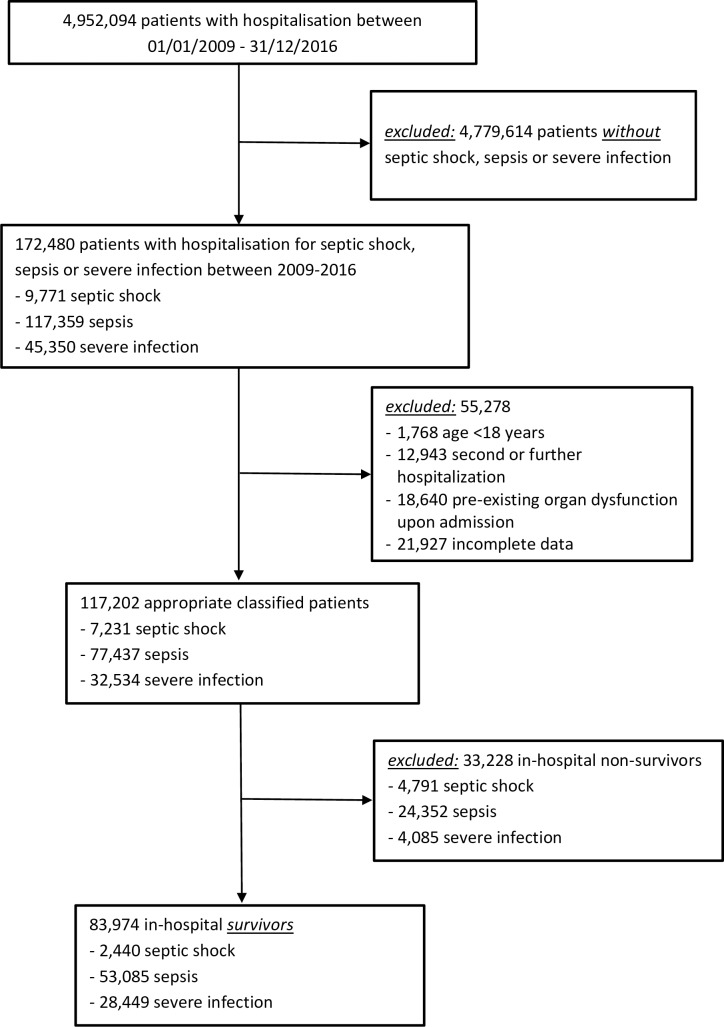
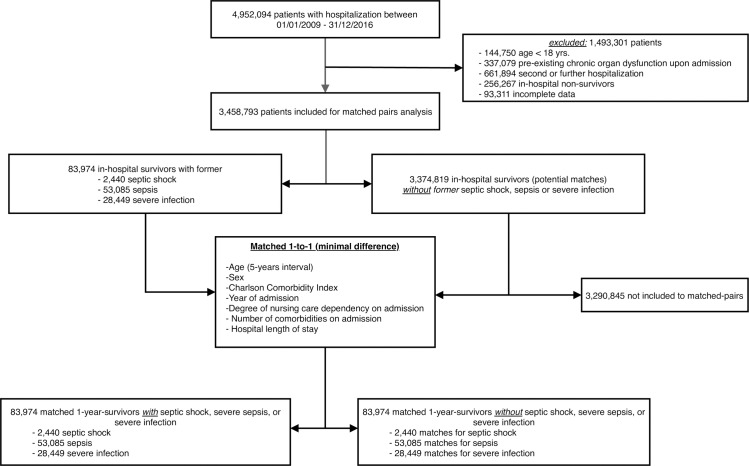
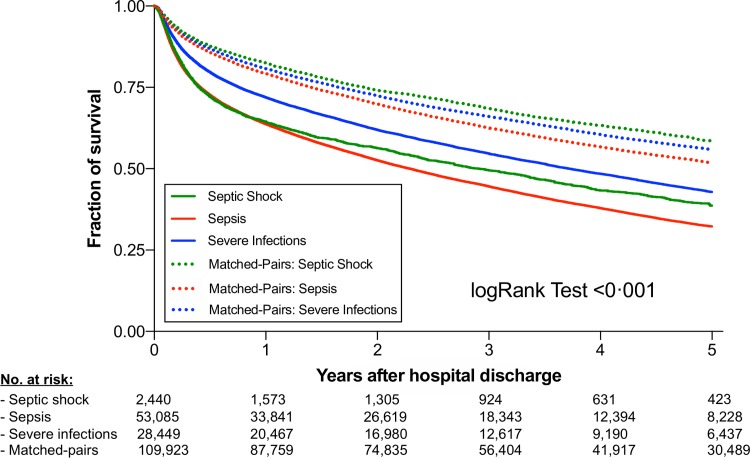
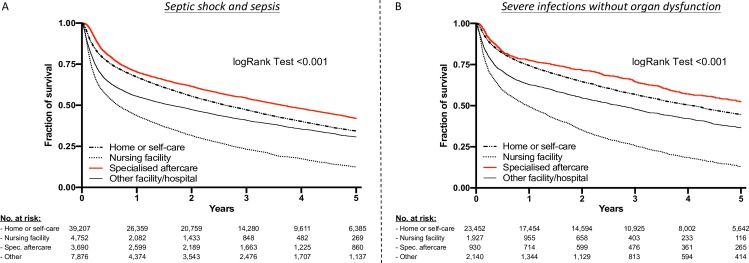
Patients with severe infections and especially sepsis have a high in-hospital mortality, but even hospital survivors face long-term sequelae, decreased health-related quality of life, and high risk of death, suggesting a great need for specialized aftercare. However, data regarding a potential benefit of post-discharge rehabilitation in these patients are scarce. In this retrospective matched cohort study the claim data of a large German statutory health care insurer was analyzed. 83,974 hospital survivors having suffered from septic shock, sepsis, and severe infections within the years 2009-2016 were identified using an ICD abstraction strategy closely matched to the current Sepsis-3 definition. Cases were analyzed and compared with their matched pairs to determine their 5-year mortality and the impact of post-discharge rehabilitation. Five years after hospital discharge, mortality of initial hospital survivors were still increased after septic shock (HRadj 2.03, 95%-CI 1.87 to 2.19; P<0.001), sepsis (HRadj 1.73, 95%-CI 1.71 to 1.76; P<0.001), and also in survivors of severe infections without organ dysfunction (HRadj 1.70, 95%-CI 1.65 to 1.74; P<0.001) compared to matched controls without infectious diseases. Strikingly, patients treated in rehabilitation facilities showed a significantly improved 5-year survival after suffering from sepsis or septic shock (HRadj 0.81, 95%-CI 0.77 to 0.85; P<0.001) as well as severe infections without organ dysfunction (HRadj 0.81, 95%-CI 0.73 to 0.90; P<0.001) compared to matched patients discharged to home or self-care. Long-term mortality and morbidity of hospital survivors are markedly increased after septic shock, sepsis and severe infections without organ dysfunction, but best 5-year survival was recorded in patients discharged to a rehabilitation facility in all three groups. Thus, our data suggest that specialized aftercare programs may help to improve long-term outcome in these patients and warrants more vigilance in future investigations.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
