

The Modified Response Evaluation Criteria in Solid Tumors (RECIST) Yield a More Accurate Prognoses Than the RECIST 1.1 in Hepatocellular Carcinoma Treated with Transarterial Radioembolization
- PMID: 32050313
- PMCID: PMC7667935
- DOI: 10.5009/gnl19197
The Modified Response Evaluation Criteria in Solid Tumors (RECIST) Yield a More Accurate Prognoses Than the RECIST 1.1 in Hepatocellular Carcinoma Treated with Transarterial Radioembolization
Abstract
Background/aims: The Response Evaluation Criteria in Solid Tumors (RECIST) 1.1 and modified RECIST (mRECIST) criteria have been used to assess treatment responses for hepatocellular carcinoma (HCC) patients. We investigated which criteria provides better survival predictions in HCC patients treated with transarterial radioembolization (TARE).
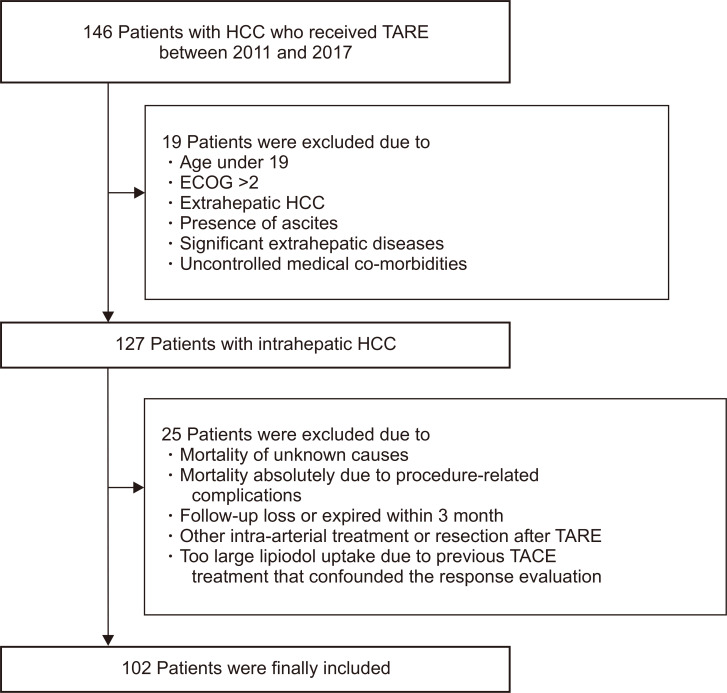
Methods: In total, 102 patients with unresectable intrahepatic HCC, who were treated with TARE between 2012 and 2017, were reviewed retrospectively. The treatment response after TARE was evaluated at 1, 3, and 6 months by the mRECIST and RECIST 1.1. Responders were defined as patients with complete or partial responses by each criterion.
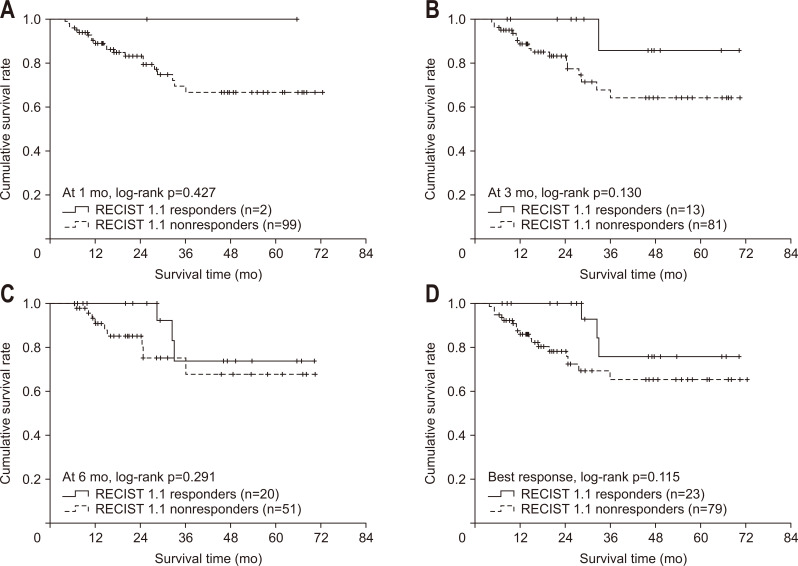
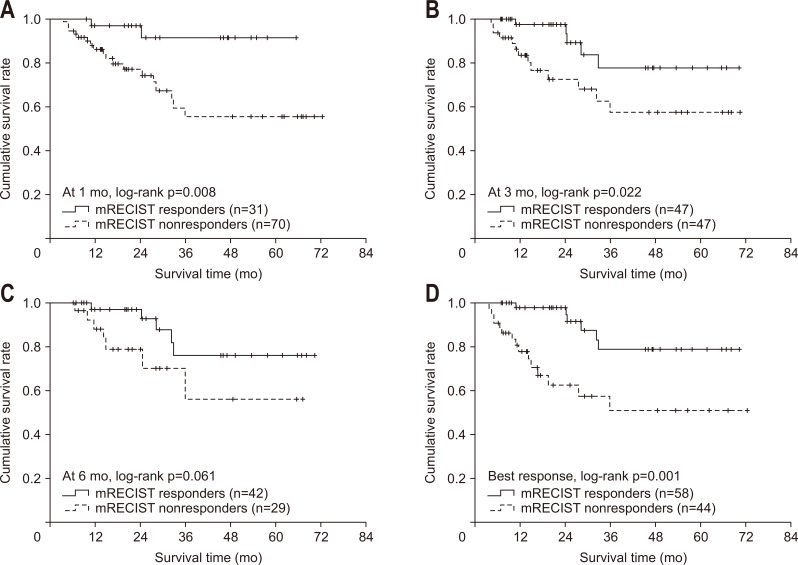
Results: The median age of 83 men and 19 women was 64.3 years. The median alpha-fetoprotein and des-gamma-carboxy prothrombin levels were 37.1 ng/mL and 1,780.0 mAU/mL, respectively. The median maximal tumor size was 8.3 cm, and multiple tumors were observed in 36 patients (35.3%). During the follow-up period (median, 20.7 months), 21 patients (20.6%) died, with a mean survival time of 55.5 months. The cumulative survival rate was 96.1% at 6 months and 89.3% at 12 months. Responders, defined by the mRECIST at 1, 3, and 6 months after TARE, showed better survival outcomes than nonresponders (hazard ratio [HR]=5.736, p=0.008 at 1 month; HR=3.145, p=0.022 at 3 months, and HR=2.887, p=0.061 at 6 months). The survival rates of responders and nonresponders defined by the RECIST 1.1 were similar (all p>0.05).
Conclusions: Response evaluations that use the mRECIST provide more accurate prognoses than those that use the RECIST 1.1 in HCC patients treated with TARE.
Keywords: Carcinoma; Embolization; Radiotherapy; Response Evaluation Criteria in Solid Tumors; Treatment outcome; hepatocellular; therapeutics.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
Comment in
-
Selecting the Right Tool for the Right Job: Which Response Criteria Better Predicts Survival of Patients Treated with Transarterial Radioembolization?Gut Liver. 2020 Nov 15;14(6):671-672. doi: 10.5009/gnl20324. Gut Liver. 2020. PMID: 33191309 Free PMC article. No abstract available.
References
-
- Sotiropoulos GC, Lang H, Frilling A, et al. Resectability of hepatocellular carcinoma: evaluation of 333 consecutive cases at a single hepatobiliary specialty center and systematic review of the literature. Hepatogastroenterology. 2006;53:322–329. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
