

Outcomes Associated with First-Line anti-PD-1/ PD-L1 agents vs. Sunitinib in Patients with Sarcomatoid Renal Cell Carcinoma: A Systematic Review and Meta-Analysis
- PMID: 32050629
- PMCID: PMC7072485
- DOI: 10.3390/cancers12020408
Outcomes Associated with First-Line anti-PD-1/ PD-L1 agents vs. Sunitinib in Patients with Sarcomatoid Renal Cell Carcinoma: A Systematic Review and Meta-Analysis
Abstract
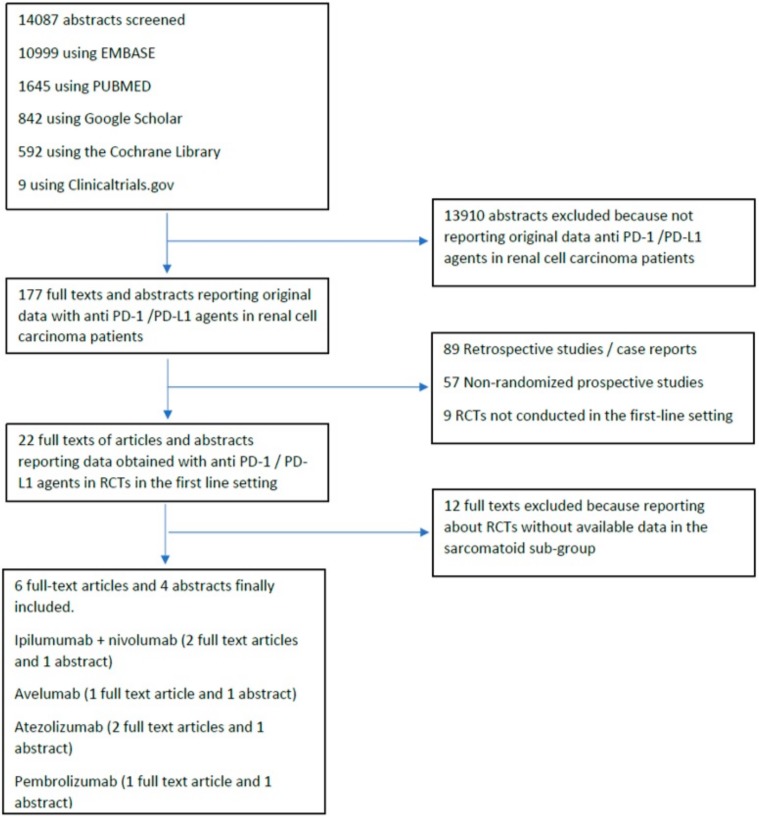
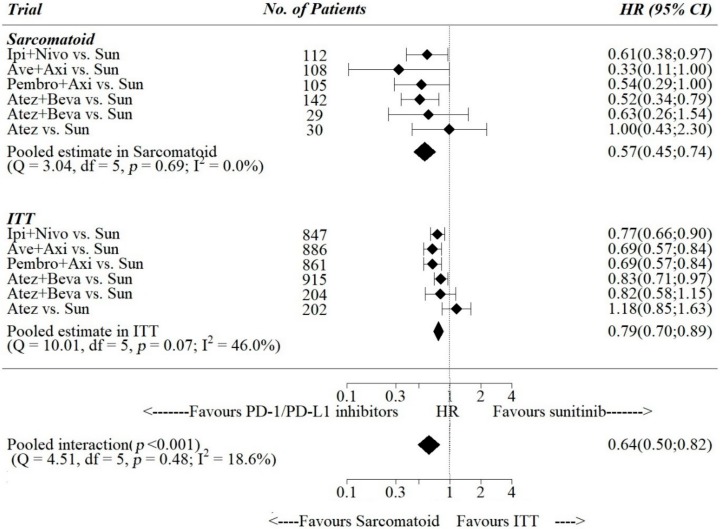
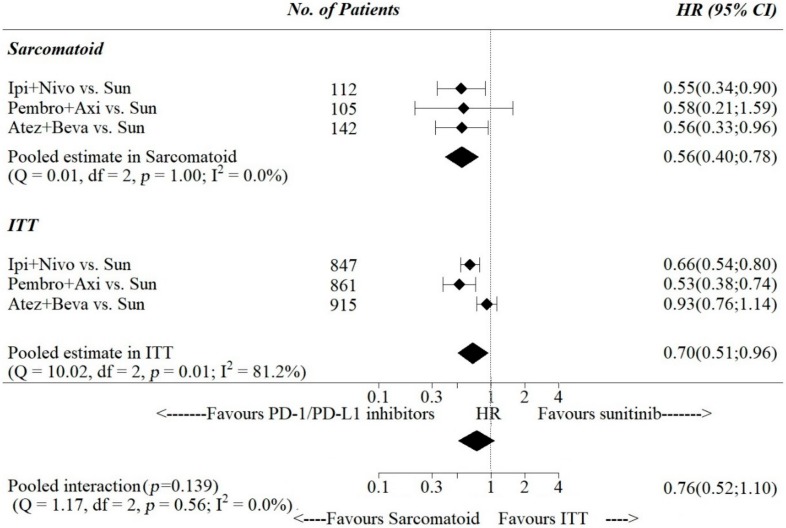
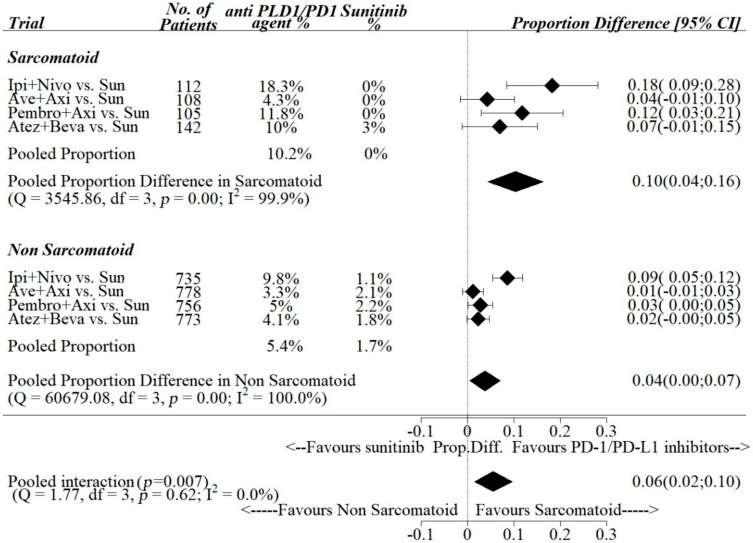
: Immunotherapy based on anti PD-1/PD-L1 inhibitors has proven to be more effective than sunitinib in the first-line setting of advanced renal cell carcinoma (RCC). RCC patients with sarcomatoid histology (sRCC) have a poor prognosis and limited therapeutic options. We performed a systematic review and a meta-analysis of randomized-controlled trials (RCTs) of first-line anti PD-1/PDL-1 agents vs. sunitinib, presenting efficacy data in the sub-group of sRCC patients. The systematic research was conducted on Google Scholar, Cochrane Library, PubMed and Embase and updated until 31th January, 2020. Abstracts from ESMO and ASCO (2010-2019) were also reviewed. Full texts and abstracts reporting about RCTs testing first-line anti-PD-1/ PD-L1 agents vs. sunitinib in RCC were included if sRCC sub-group analyses of either PFS (progression-free survival), OS (overall survival) or radiological response rate were available. Pooled data from 3814 RCC patients in the ITT (intention-to-treat) population and from 512 sRCC patients were included in the quantitative synthesis. In the sRCC sub-group vs. the ITT population, pooled estimates of the PFS-HRs were 0.57 (95%: 0.45-0.74) vs. 0.79 (95% CI: 0.70-0.89), respectively, with a statistically meaningful interaction favoring the sRCC sub-group (pooled ratio of the PFS-HRs = 0.64; 95% CI: 0.50-0.82; p < 0.001). Pooled estimates of the difference in CR-R (complete response-rate) achieved with anti-PD-1/PDL-1 agents vs. sunitinib were + 0.10 (95% CI: 0.04-0.16) vs. + 0.04 (95% CI: 0.00-0.07) in the sRCC vs. the non-sRCC sub groups, with a statistically meaningful difference of + 0.06 (95% CI: 0.02-0.10; p = 0.007) favoring the sRCC sub-group. Sarcomatoid histology may be associated with improved efficacy of anti PD-1/PDL-1 agents vs. sunitinib in terms of PFS and CR-R.
Keywords: PD-1; PD-L1; immune checkpoint inhibitors; renal cell carcinoma; sarcomatoid.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Kidney Cancer Statistics. [(accessed on 10 January 2020)]; Available online: https://www.wcrf.org/dietandcancer/cancer-trends/kidney-cancer-statistics.
-
- Wang J., Li X., Wu X., Wang Z., Zhang C., Cao G., Zhang X., Peng F., Yan T. Role of immune checkpoint inhibitor-based therapies for metastatic renal cell carcinoma in the first-line setting: A Bayesian network analysis. EBioMedicine. 2019;47:78–88. doi: 10.1016/j.ebiom.2019.08.006. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
