

Annual and seasonal patterns in etiologies of pediatric community-acquired pneumonia due to respiratory viruses and Mycoplasma pneumoniae requiring hospitalization in South Korea
- PMID: 32050912
- PMCID: PMC7017508
- DOI: 10.1186/s12879-020-4810-9
Annual and seasonal patterns in etiologies of pediatric community-acquired pneumonia due to respiratory viruses and Mycoplasma pneumoniae requiring hospitalization in South Korea
Abstract
Background: Community-acquired pneumonia (CAP) is one of the leading worldwide causes of childhood morbidity and mortality. Its disease burden varies by age and etiology and is time dependent. We aimed to investigate the annual and seasonal patterns in etiologies of pediatric CAP requiring hospitalization.
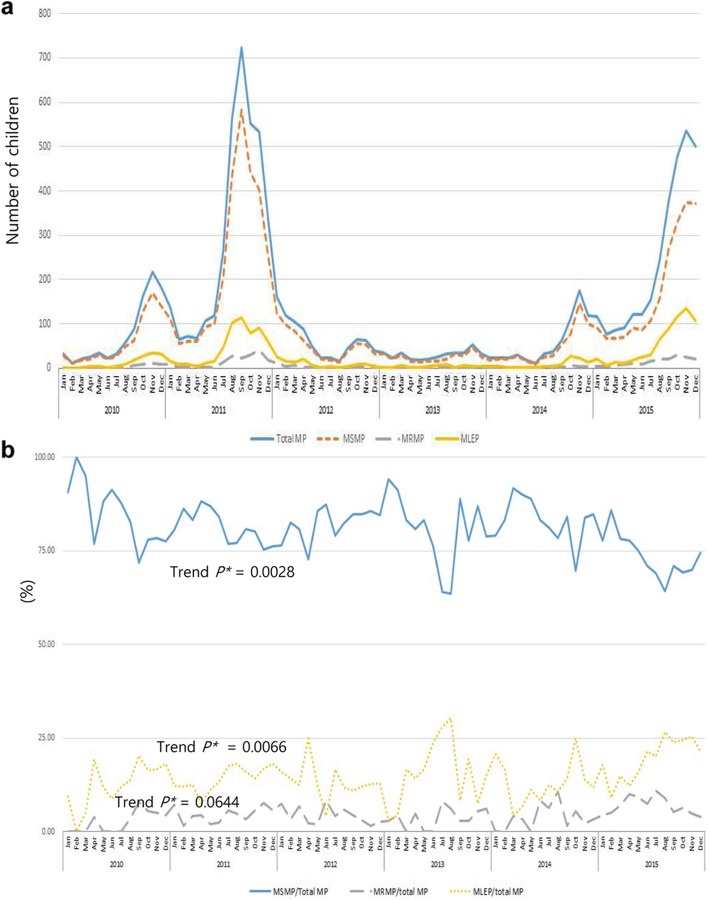
Methods: We conducted a retrospective study in 30,994 children (aged 0-18 years) with CAP between 2010 and 2015 at 23 nationwide hospitals in South Korea. Mycoplasma pneumoniae (MP) pneumonia was clinically classified as macrolide-sensitive MP, macrolide-less effective MP (MLEP), and macrolide-refractory MP (MRMP) based on fever duration after initiation of macrolide treatment, regardless of the results of in vitro macrolide sensitivity tests.
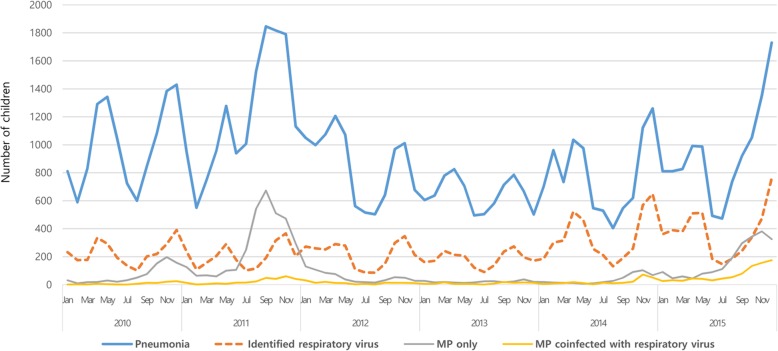
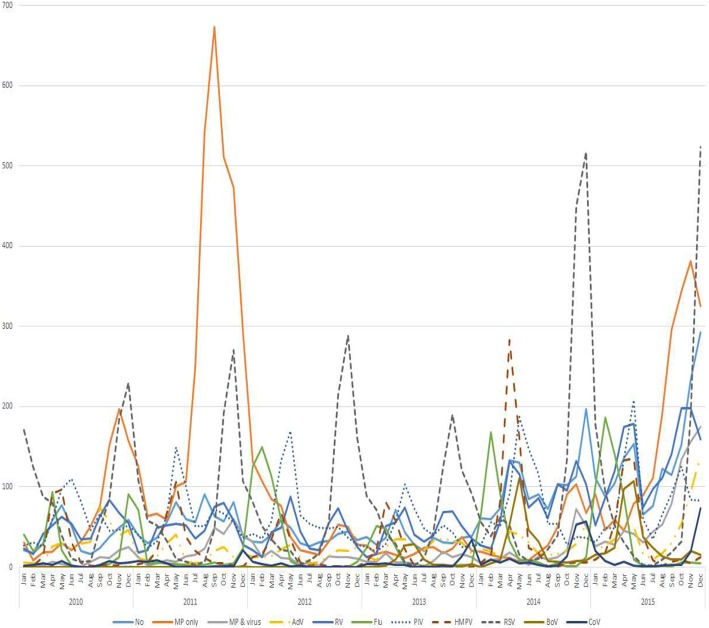
Results: MP and respiratory syncytial virus (RSV) were the two most commonly identified pathogens of CAP. With the two epidemics of MP pneumonia (2011 and 2015), the rates of clinical MLEP and MRMP pneumonia showed increasing trends of 36.4% of the total MP pneumonia. In children < 2 years of age, RSV (34.0%) was the most common cause of CAP, followed by MP (9.4%); however, MP was the most common cause of CAP in children aged 2-18 years of age (45.3%). Systemic corticosteroid was most commonly administered for MP pneumonia. The rate of hospitalization in intensive care units was the highest for RSV pneumonia, and ventilator care was most commonly needed in cases of adenovirus pneumonia.
Conclusions: The present study provides fundamental data to establish public health policies to decrease the disease burden due to CAP and improve pediatric health.
Keywords: Children; Macrolide less-effective; Macrolide- refractory; Macrolide-sensitive; Mycoplasma pneumoniae; Pneumonia; Respiratory virus.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Global Burden of Disease Pediatrics Collaboration. Kyu HH, Pinho C, Wagner JA, Brown JC, Bertozzi-Villa A, Charlson FJ, Coffeng LE, Dandona L, Erskine HE, et al. Global and national burden of diseases and injuries among children and adolescents between 1990 and 2013: findings from the global burden of disease 2013 study. JAMA Pediatr. 2016;170(3):267–287. doi: 10.1001/jamapediatrics.2015.4276. - DOI - PMC - PubMed
-
- GBD 2015 LRI Collaborators Estimates of the global, regional, and national morbidity, mortality, and aetiologies of lower respiratory tract infections in 195 countries: a systematic analysis for the global burden of disease study 2015. Lancet Infect Dis. 2017;17(11):1133–1161. doi: 10.1016/S1473-3099(17)30396-1. - DOI - PMC - PubMed
-
- Shi T, McAllister DA, O'Brien KL, Simoes EAF, Madhi SA, Gessner BD, Polack FP, Balsells E, Acacio S, Aguayo C, et al. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in young children in 2015: a systematic review and modelling study. Lancet. 2017;390(10098):946–958. doi: 10.1016/S0140-6736(17)30938-8. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
