

Phenotypic comparison between smoking and non-smoking chronic obstructive pulmonary disease
- PMID: 32050955
- PMCID: PMC7017521
- DOI: 10.1186/s12931-020-1310-9
Phenotypic comparison between smoking and non-smoking chronic obstructive pulmonary disease
Abstract
Background: Although COPD among non-smokers (NS-COPD) is common, little is known about this phenotype. We compared NS-COPD subjects with smoking COPD (S-COPD) patients in a rural Indian population using a variety of clinical, physiological, radiological, sputum cellular and blood biomarkers.
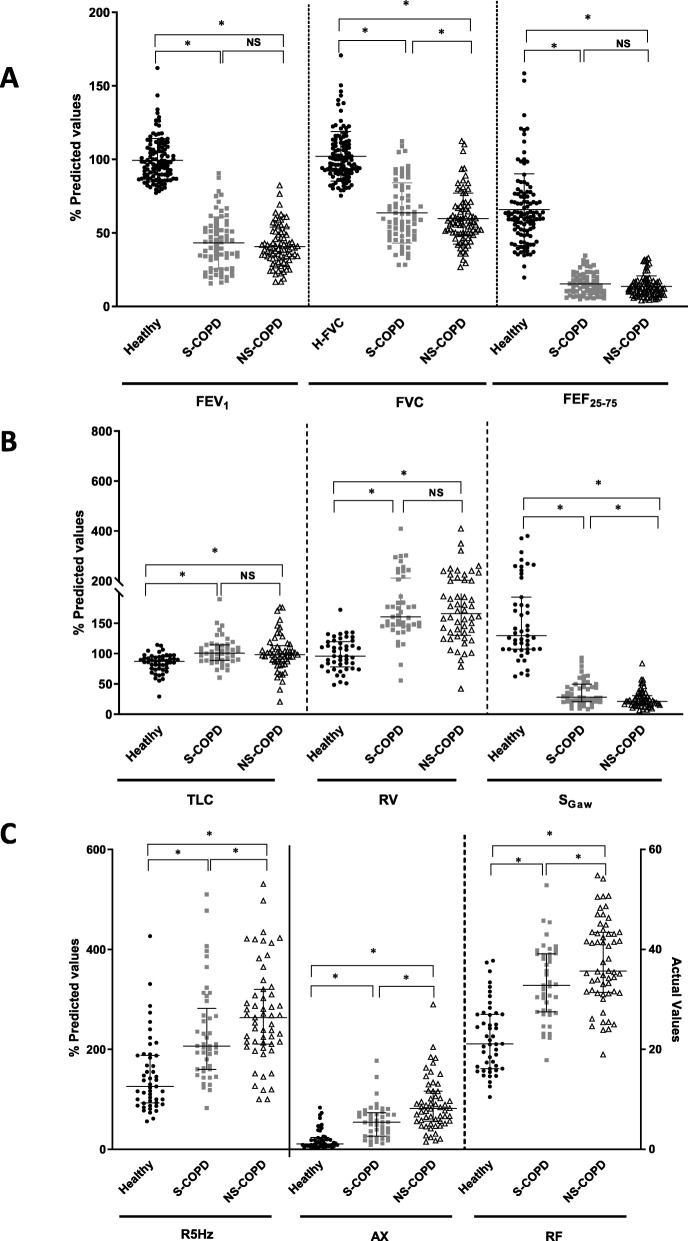
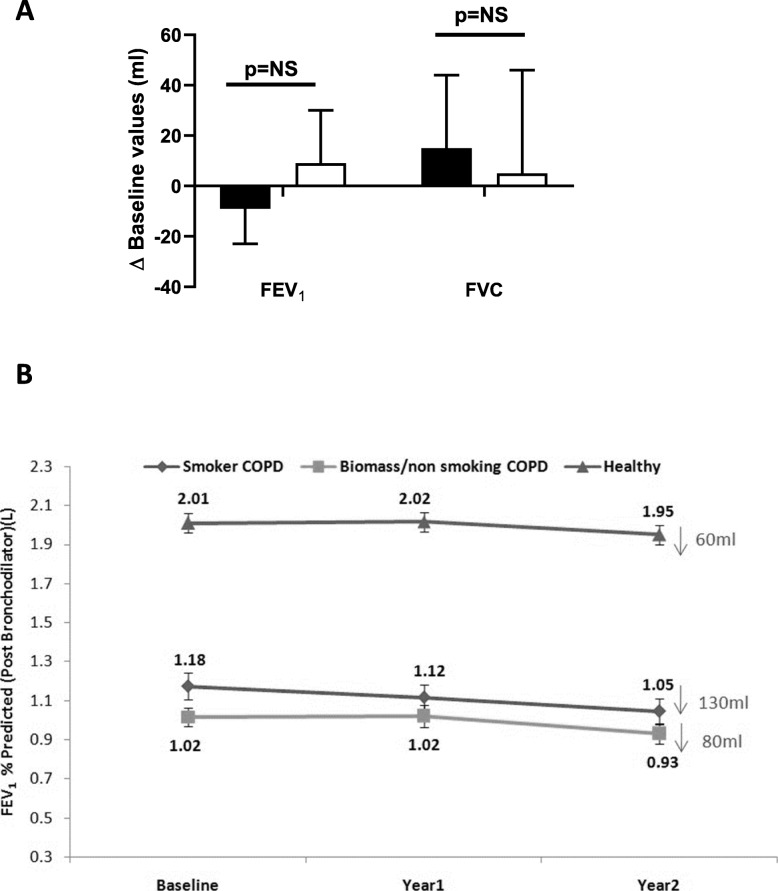
Methods: Two hundred ninety subjects (118 healthy, 79 S-COPD, 93 NS-COPD) performed pre- and post-bronchodilator spirometry and were followed for 2 years to study the annual rate of decline in lung function. Body plethysmography, impulse oscillometry, inspiratory-expiratory HRCT, induced sputum cellular profile and blood biomarkers were compared between 49 healthy, 45 S-COPD and 55 NS-COPD subjects using standardized methods. Spirometric response to oral corticosteroids was measured in 30 female NS-COPD patients.
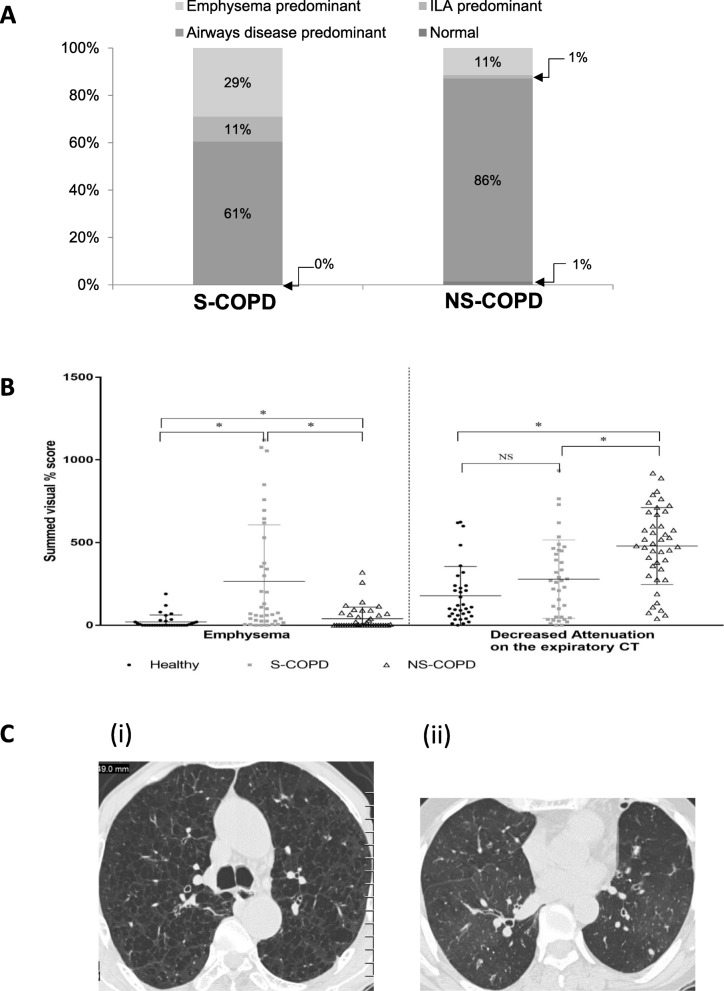
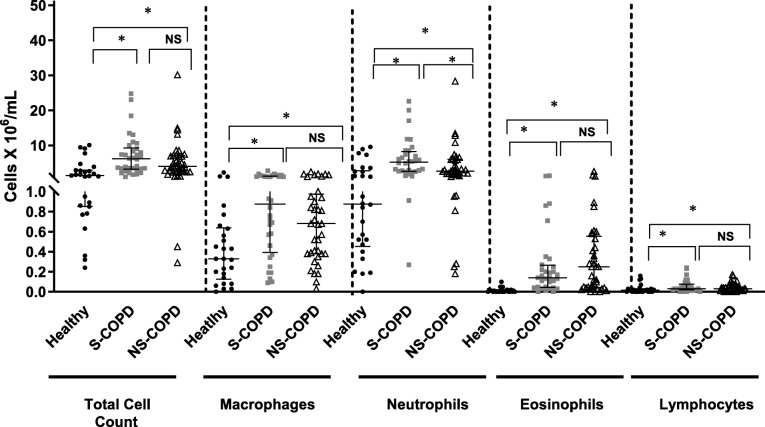
Results: Compared to all male S-COPD subjects, 47% of NS-COPD subjects were female, were younger by 3.2 years, had greater body mass index, a slower rate of decline in lung function (80 vs 130 mL/year), more small airways obstruction measured by impulse oscillometry (p < 0.001), significantly less emphysema (29% vs 11%) on CT scans, lower values in lung diffusion parameters, significantly less neutrophils in induced sputum (p < 0.05) and tended to have more sputum eosinophils. Hemoglobin and red cell volume were higher and serum insulin lower in S-COPD compared to NS-COPD. Spirometric indices, symptoms and quality of life were similar between S-COPD and NS-COPD. There was no improvement in spirometry in NS-COPD patients after 2 weeks of an oral corticosteroid.
Conclusions: Compared to S-COPD, NS-COPD is seen in younger subjects with equal male-female predominance, is predominantly a small-airway disease phenotype with less emphysema, preserved lung diffusion and a slower rate of decline in lung function.
Keywords: Chronic obstructive pulmonary disease; biomass smoke; household air pollution; non-smoking COPD; small airway disease.
Conflict of interest statement
PB and LD receive research funding from AstraZeneca and Boehringer-Ingelheim, PB receives funding for scientific advisory boards and travel from AstraZeneca, Boehringer- Ingelheim, Novartis, Teva and Pieris. The other authors have no competing interests to declare.
Figures
References
-
- Collaborators GCRD Global, regional, and national deaths, prevalence, disability-adjusted life years, and years lived with disability for chronic obstructive pulmonary disease and asthma, 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet Respir Med. 2017;5:691–706. doi: 10.1016/S2213-2600(17)30293-X. - DOI - PMC - PubMed
-
- Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V, Abraham J, Adair T, Aggarwal R, Ahn SY, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380:2095–2128. doi: 10.1016/S0140-6736(12)61728-0. - DOI - PMC - PubMed
-
- World Health Organisation . Chronic obstructive pulmonary disease. 2018.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
