

Novel Detection and Restorative Levodopa Treatment for Preclinical Diabetic Retinopathy
- PMID: 32051147
- PMCID: PMC7306127
- DOI: 10.2337/db19-0869
Novel Detection and Restorative Levodopa Treatment for Preclinical Diabetic Retinopathy
Abstract
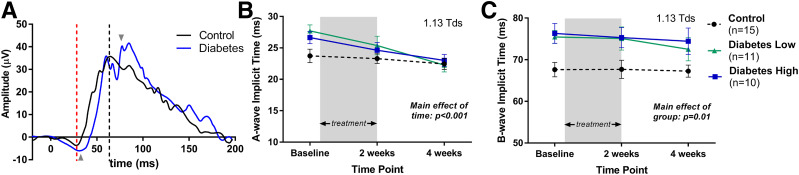
Diabetic retinopathy (DR) is diagnosed clinically by directly viewing retinal vascular changes during ophthalmoscopy or through fundus photographs. However, electroretinography (ERG) studies in humans and rodents have revealed that retinal dysfunction is demonstrable prior to the development of visible vascular defects. Specifically, delays in dark-adapted ERG oscillatory potential (OP) implicit times in response to dim-flash stimuli (<-1.8 log cd · s/m2) occur prior to clinically recognized DR. Animal studies suggest that retinal dopamine deficiency underlies these early functional deficits. In this study, we randomized individuals with diabetes, without clinically detectable retinopathy, to treatment with either low- or high-dose Sinemet (levodopa plus carbidopa) for 2 weeks and compared their ERG findings with those of control subjects (no diabetes). We assessed dim-flash-stimulated OP delays using a novel handheld ERG system (RETeval) at baseline and 2 and 4 weeks. RETeval recordings identified significant OP implicit time delays in individuals with diabetes without retinopathy compared with age-matched control subjects (P < 0.001). After 2 weeks of Sinemet treatment, OP implicit times were restored to control values, and these improvements persisted even after a 2-week washout. We conclude that detection of dim-flash OP delays could provide early detection of DR and that Sinemet treatment may reverse retinal dysfunction.
Trial registration: ClinicalTrials.gov NCT02706977.
© 2020 by the American Diabetes Association.
Figures





Comment in
-
Dopamine and Early Retinal Dysfunction in Diabetes: Insights From a Phase 1 Study.Diabetes. 2020 Jul;69(7):1339-1340. doi: 10.2337/dbi20-0009. Epub 2020 Apr 20. Diabetes. 2020. PMID: 32312866 No abstract available.
References
-
- Cho NH, Shaw JE, Karuranga S, et al. IDF Diabetes Atlas: global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res Clin Pract 2018;138:271–281 - PubMed
-
- Stefánsson E, Bek T, Porta M, Larsen N, Kristinsson JK, Agardh E. Screening and prevention of diabetic blindness. Acta Ophthalmol Scand 2000;78:374–385 - PubMed
-
- Frank RN. Diabetic retinopathy. N Engl J Med 2004;350:48–58 - PubMed
-
- Sharma S, Oliver-Fernandez A, Liu W, Buchholz P, Walt J. The impact of diabetic retinopathy on health-related quality of life. Curr Opin Ophthalmol 2005;16:155–159 - PubMed
-
- Gross JG, Glassman AR, Liu D, et al.; Diabetic Retinopathy Clinical Research Network . Five-year outcomes of panretinal photocoagulation vs intravitreous ranibizumab for proliferative diabetic retinopathy: a randomized clinical trial [published correction appears in JAMA Ophthalmol 2019;137:467]. JAMA Ophthalmol 2018;136:1138–1148 - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
