

A Multi-Institutional Cohort of Therapy-Associated Polyposis in Childhood and Young Adulthood Cancer Survivors
- PMID: 32051178
- PMCID: PMC7060102
- DOI: 10.1158/1940-6207.CAPR-19-0416
A Multi-Institutional Cohort of Therapy-Associated Polyposis in Childhood and Young Adulthood Cancer Survivors
Abstract
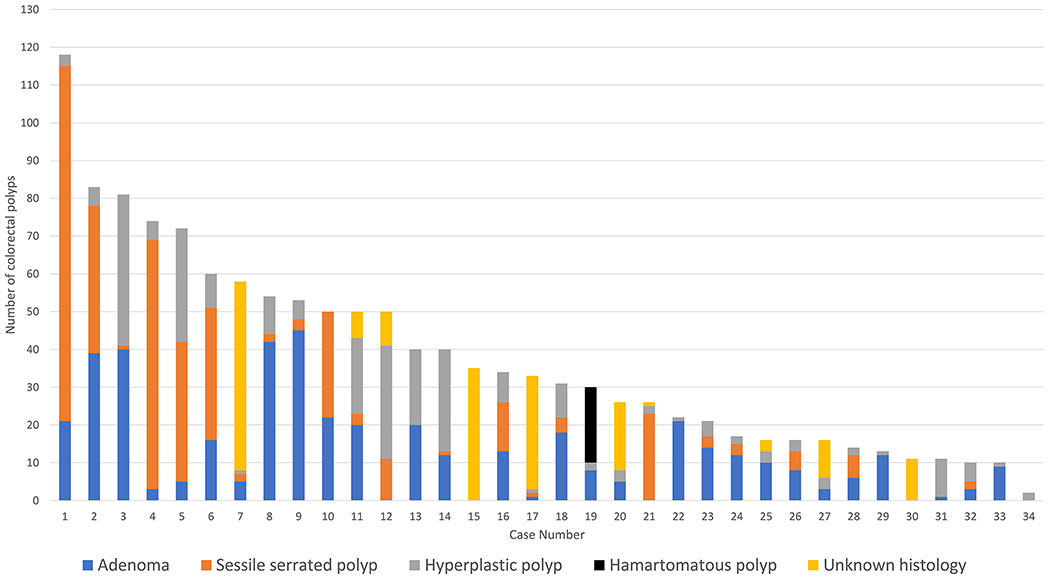
Prior small reports have postulated a link between gastrointestinal polyposis and childhood and young adulthood cancer (CYAC) treatment (therapy-associated polyposis; TAP), but this remains a poorly understood phenomenon. The aim of this study was to describe the phenotypic spectrum of TAP in a multi-institutional cohort. TAP cases were identified from eight high-risk cancer centers. Cases were defined as patients with ≥10 gastrointestinal polyps without known causative germline alteration or hereditary colorectal cancer predisposition syndrome who had a history of prior treatment with chemotherapy and/or radiotherapy for CYAC. A total of 34 TAP cases were included (original CYAC: 27 Hodgkin lymphoma, three neuroblastoma, one acute myeloid leukemia, one medulloblastoma, one nephroblastoma, and one non-Hodgkin lymphoma). Gastrointestinal polyposis was first detected at a median of 27 years (interquartile range, 20-33) after CYAC treatment. A total of 12 of 34 (35%) TAP cases had ≥50 colorectal polyps. A total of 32 of 34 (94%) had >1 histologic polyp type. A total of 25 of 34 (74%) had clinical features suggestive of ≥1 colorectal cancer predisposition syndrome [e.g., attenuated familial adenomatous polyposis (FAP), serrated polyposis syndrome, extracolonic manifestations of FAP, mismatch repair-deficient colorectal cancer, or hamartomatous polyposis] including 8 of 34 (24%) with features of multiple such syndromes. TAP is an apparently acquired phenomenon that should be considered in patients who develop significant polyposis without known causative germline alteration but who have had prior treatment for a CYAC. Patients with TAP have features that may mimic various hereditary colorectal cancer syndromes, suggesting multiple concurrent biologic mechanisms, and recognition of this diagnosis may have implications for cancer risk and screening.
©2020 American Association for Cancer Research.
Conflict of interest statement
LHB: no conflict of interest to report
CU: no conflict of interest to report
TGD: no conflict of interest to report
CAB: no conflict of interest to report
YC: no conflict of interest to report
AC: no conflict of interest to report
JMC: no conflict of interest to report
ESK: no conflict of interest to report
BHL: Advisory Board: Invitae, Speakers Bureau Myriad Genetics Lab
EL: no conflict of interest to report
RML: no conflict of interest to report
ML: no conflict of interest to report
ESM: no conflict of interest to report
RS: no conflict of interest to report
GI: no conflict of interest to report
FK: no conflict of interest to report
ES: no conflict of interest to report
JMW: no conflict of interest to report
MJH: no conflict of interest to report
MFK: no conflict of interest to report
ZKS: Immediate Family Member, Ophthalmology: Consulting/Advisory Role: Allergan, Adverum Biotechnologies, Alimera Sciences, Biomarin, Fortress Biotech, Genentech, Novartis, Optos, Regeneron, Regenxbio, Spark Therapeutics
SS: consultant for Myriad Genetics and Digital China Health Technologies and has rights to an inventor portion of the licensing revenue from PREMM5
MBY: no conflicts of interest to report
Figures
References
-
- Reulen RC, Frobisher C, Winter DL, Kelly J, Lancashire ER, Stiller CA, et al. Long-term risks of subsequent primary neoplasms among survivors of childhood cancer. JAMA. 2011;305(22):2311–2319. - PubMed
-
- Teepen JC, Kok JL, van Leeuwen FE, Tissing WJE, Dolsma W V, van der Pal HJ, et al. Colorectal Adenomas and Cancers After Childhood Cancer Treatment: A DCOG-LATER Record Linkage Study. JNCI J Natl Cancer Inst. 2018;110(7):758–767. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
