

Natural History of Nonalcoholic Fatty Liver Disease: Implications for Clinical Practice and an Individualized Approach
- PMID: 32051820
- PMCID: PMC6995480
- DOI: 10.1155/2020/9181368
Natural History of Nonalcoholic Fatty Liver Disease: Implications for Clinical Practice and an Individualized Approach
Abstract
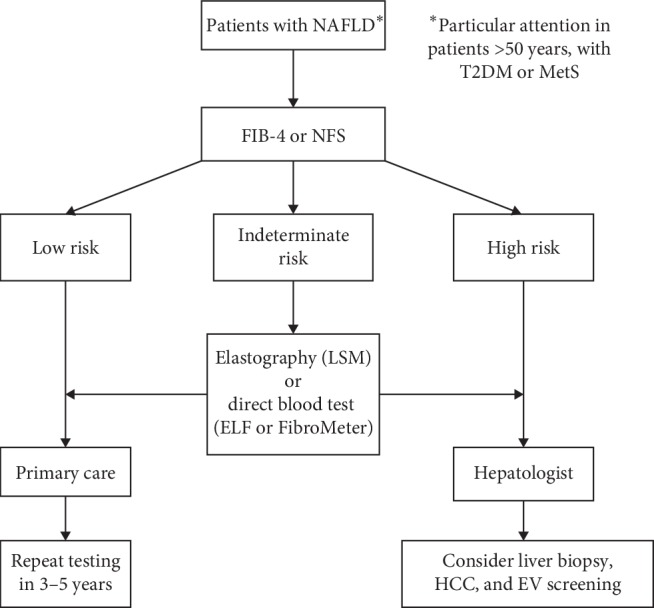
Nonalcoholic fatty liver disease (NAFLD) is becoming the most prevalent liver disease worldwide, associated with epidemics of overweight and resulting metabolic syndrome (MetS). Around 20-30% of patients with NAFLD develop progressive liver fibrosis, which is the most important predictor of liver-related and overall morbidity and mortality. In contrast to classical understanding, no significant association has been demonstrated between the inflammatory component of NAFLD, i.e., nonalcoholic steatohepatitis (NASH), and the adverse clinical outcomes. Older age (>50 years) and presence of type 2 diabetes mellitus, in addition to some genetic variants, are most consistently reported indicators of increased risk of having liver fibrosis. However, critical driving force for the progression of fibrosis and risk factors for this have still not been fully elucidated. Apart from the genetic profile, gut dysbiosis, weight gain, worsening of insulin resistance, and worsening of liver steatosis represent candidate factors associated with unfavourable development of liver disease. Cardiovascular events, extrahepatic malignancies, and liver-related deaths are the leading causes of mortality in NAFLD. As patients with advanced fibrosis are under highest risk of adverse clinical outcomes, efforts should be made to recognize individuals under risk and rule out the presence of this stage of fibrosis, preferably by using simple noninvasive tools. This process should start at the primary care level by using validated biochemical tests, followed by direct serum tests for fibrosis or elastography in the remaining patients. Patients with advanced fibrosis should be referred to hepatologists for aggressive lifestyle modification and correction of the components of MetS, and cirrhotic patients should be screened for hepatocellular carcinoma and oesophageal varices.
Copyright © 2020 Ivica Grgurevic et al.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
