

Radiation Therapy Practice Patterns for Brain Metastases in the United States in the Stereotactic Radiosurgery Era
- PMID: 32051889
- PMCID: PMC7004940
- DOI: 10.1016/j.adro.2019.07.012
Radiation Therapy Practice Patterns for Brain Metastases in the United States in the Stereotactic Radiosurgery Era
Abstract
Purpose: Utilization of stereotactic radiosurgery (SRS) for brain metastases (BM) has increased, prompting reassessment of whole brain radiation therapy (WBRT). A pattern of care analysis of SRS and WBRT dose-fractionations was performed in patients presenting with BM at the time of cancer diagnosis.
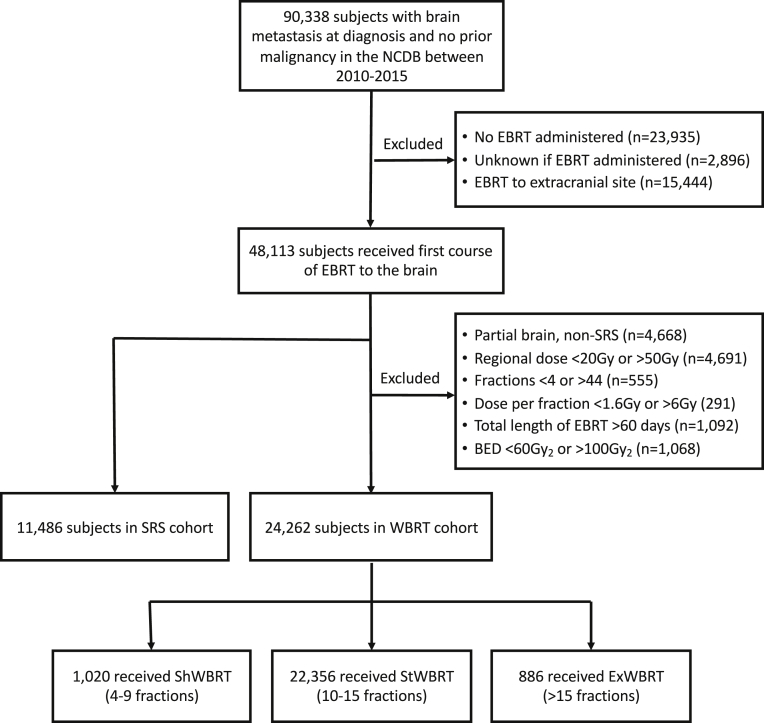
Methods and materials: Adults with BM at cancer diagnosis between 2010 to 2015 and no prior malignancy were identified in the National Cancer Database. SRS was defined using published thresholds. Short (ShWBRT), standard (StWBRT), and extended (ExWBRT) dose-fractionations were defined as 4 to 9, 10 to 15, and >15 fractions. Radioresistant histology was defined as melanoma, renal cell carcinoma, sarcoma or spindle cell, or gastrointestinal primary.
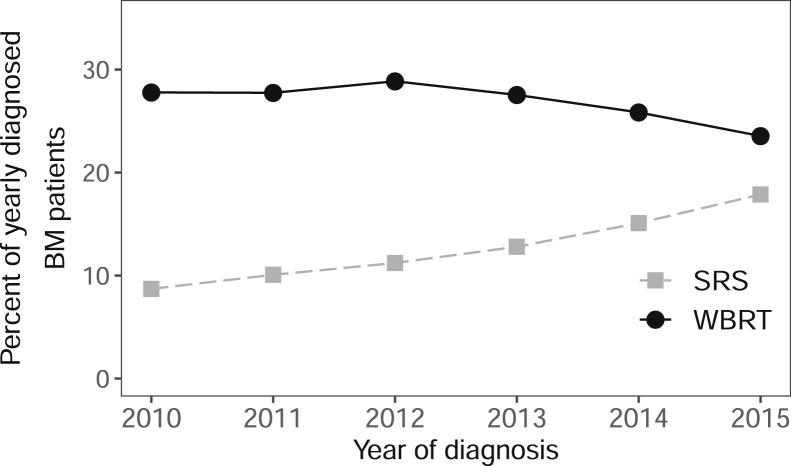
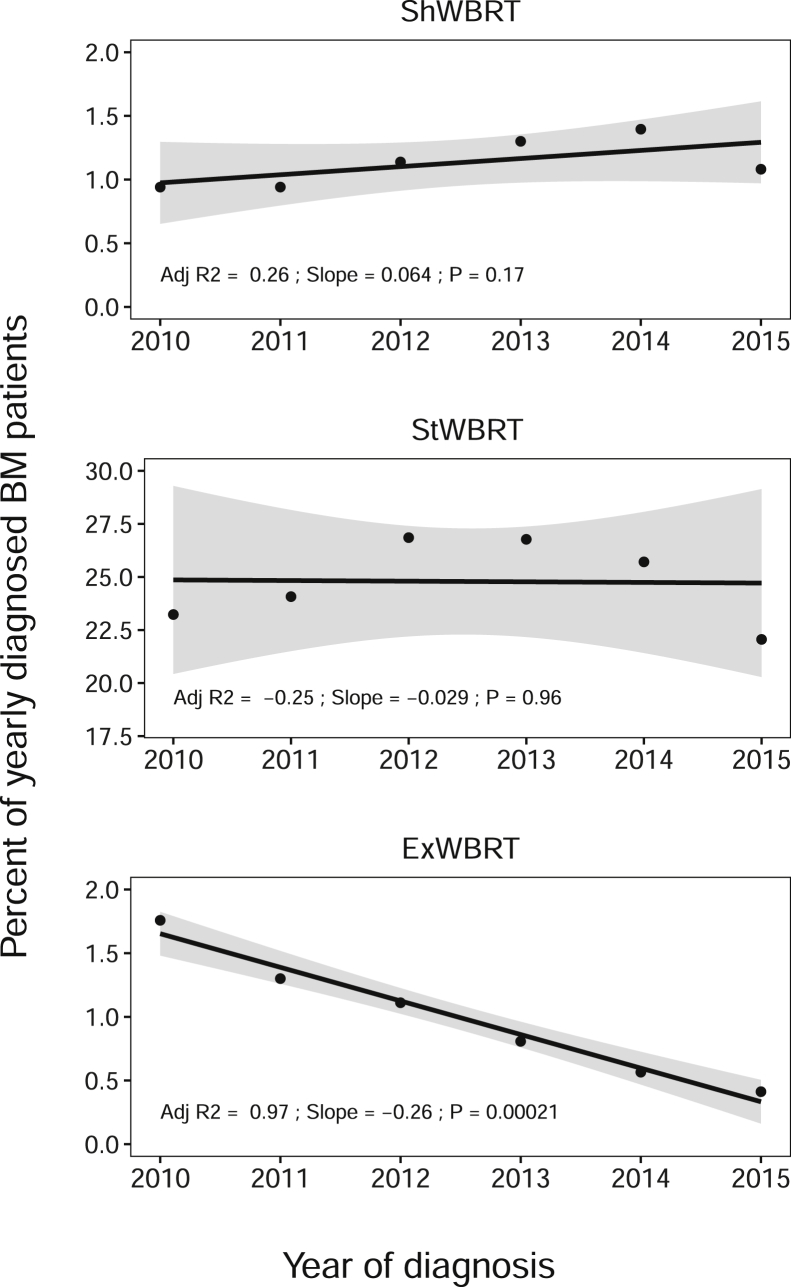
Results: Of 4,087,967 adults with their first lifetime cancer, 90,388 (2.2%) had BM at initial diagnosis. Of these, 11,486 (12.7%) received SRS and 24,262 (26.8%) WBRT as first-course radiation therapy. The proportion of annual WBRT use decreased from 27.8% to 23.5% of newly diagnosed patients, and SRS increased from 8.7% to 17.9%. Common dose-fractionations were 30 Gy in 10 fractions (56.8%) for WBRT and 20 Gy in 1 fraction (13.0%) for SRS. On multivariate analysis, factors significantly associated with SRS versus WBRT included later year of diagnosis (2015 vs 2010, adjusted odds ratio [aOR] = 2.4), radioresistance (aOR = 2.0), academic facility (aOR = 1.9), highest income quartile (aOR = 1.6), chemotherapy administration (aOR = 1.4), and longer travel distance (>15 vs < 5 miles, aOR = 1.4). Linear regression revealed significant ExWBRT reductions (-22.4%/y, R2 = 0.97, P < .001) and no significant change for ShWBRT or StWBRT. Patients were significantly more likely to receive ShWBRT than StWBRT if not treated with chemotherapy (aOR = 3.5).
Conclusions: Utilization of WBRT, particularly ExWBRT, decreased while SRS utilization doubled as the first radiation therapy course in patients with BM at diagnosis. Patients with radioresistant histologies were more likely to receive SRS. Those not receiving chemotherapy, potentially owing to poor performance status, were less likely to receive SRS and more likely to receive ShWBRT.
© 2019 The Authors.
Figures
References
-
- Nussbaum E.S., Djalilian H.R., Cho K.H., Hall W.A. Brain metastases. Histology, multiplicity, surgery, and survival. Cancer. 1996;78:1781–1788. - PubMed
-
- Chen R.C., Punglia R.S., Sher D.J. Stereotactic radiosurgery (SRS) vs. whole brain radiation therapy (WBRT) vs. combined treatment (SRS & WBRT) for brain metastases: A decision analysis. Int J Radiat Oncol Biol Phys. 2009;75:S89.
-
- Chao J.H., Phillips R., Nickson J.J. Roentgen-ray therapy of cerebral metastases. Cancer. 1954;7:682–689. - PubMed
-
- Order S.E., Hellman S., Von Essen C.F., Kligerman M.M. Improvement in quality of survival following whole-brain irradiation for brain metastasis. Radiology. 1968;91:149–153. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
