

Ischemic Stroke despite Oral Anticoagulant Therapy in Patients with Atrial Fibrillation
- PMID: 32052481
- PMCID: PMC7383617
- DOI: 10.1002/ana.25700
Ischemic Stroke despite Oral Anticoagulant Therapy in Patients with Atrial Fibrillation
Abstract
Objective: It is not known whether patients with atrial fibrillation (AF) with ischemic stroke despite oral anticoagulant therapy are at increased risk for further recurrent strokes or how ongoing secondary prevention should be managed.
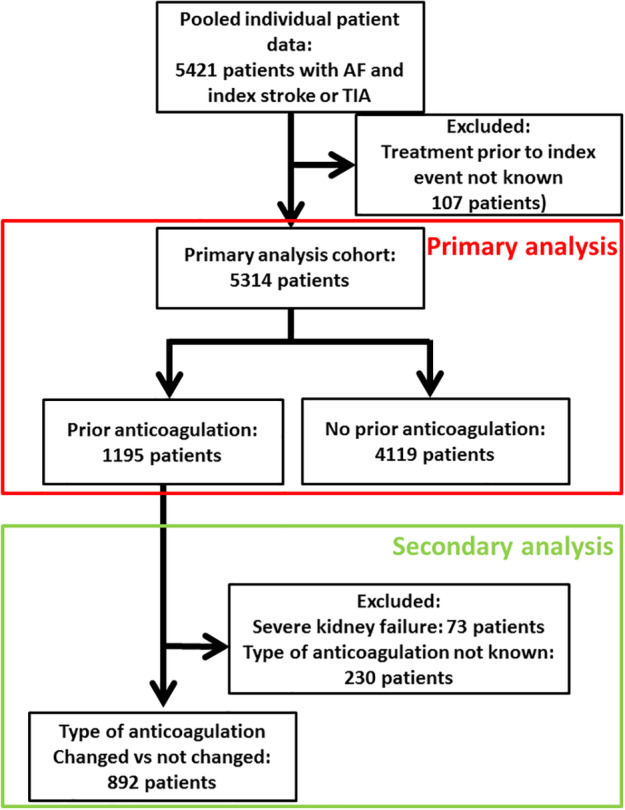
Methods: We conducted an individual patient data pooled analysis of 7 prospective cohort studies that recruited patients with AF and recent cerebral ischemia. We compared patients taking oral anticoagulants (vitamin K antagonists [VKA] or direct oral anticoagulants [DOAC]) prior to index event (OACprior ) with those without prior oral anticoagulation (OACnaive ). We further compared those who changed the type (ie, from VKA or DOAC, vice versa, or DOAC to DOAC) of anticoagulation (OACchanged ) with those who continued the same anticoagulation as secondary prevention (OACunchanged ). Time to recurrent acute ischemic stroke (AIS) was analyzed using multivariate competing risk Fine-Gray models to calculate hazard ratios (HRs) and 95% confidence intervals (CIs).
Results: We included 5,413 patients (median age = 78 years [interquartile range (IQR) = 71-84 years]; 5,136 [96.7%] had ischemic stroke as the index event, median National Institutes of Health Stroke Scale on admission = 6 [IQR = 2-12]). The median CHA2 DS2 -Vasc score (congestive heart failure, hypertension, age≥ 75 years, diabetes mellitus, stroke/transient ischemic attack, vascular disease, age 65-74 years, sex category) was 5 (IQR = 4-6) and was similar for OACprior (n = 1,195) and OACnaive (n = 4,119, p = 0.103). During 6,128 patient-years of follow-up, 289 patients had AIS (4.7% per year, 95% CI = 4.2-5.3%). OACprior was associated with an increased risk of AIS (HR = 1.6, 95% CI = 1.2-2.3, p = 0.005). OACchanged (n = 307) was not associated with decreased risk of AIS (HR = 1.2, 95% CI = 0.7-2.1, p = 0.415) compared with OACunchanged (n = 585).
Interpretation: Patients with AF who have an ischemic stroke despite previous oral anticoagulation are at a higher risk for recurrent ischemic stroke despite a CHA2 DS2 -Vasc score similar to those without prior oral anticoagulation. Better prevention strategies are needed for this high-risk patient group. ANN NEUROL 2020.
© 2020 The Authors. Annals of Neurology published by Wiley Periodicals, Inc. on behalf of American Neurological Association.
Conflict of interest statement
The following companies manufacture drugs involved in this study: Bayer (BY), Boehringer Ingelheim (BI), Pfizer/Bristol Meyer Squibb (PB), and Daiichi Sankyo (DSA). D.S.: scientific advisory boards, BY and PB. G.M.D.M.: travel honoraria, BY; speaker honoraria, PB. M.P.: honoraria for speaker bureau, BY, BI, PB, and DSA. K.Ma.: advisory boards, BI, BY, and DSA. S.T.E.: travel or speaker honoraria, BY, BI; scientific advisory boards, BY, BI, and PB; educational grant, PB. D.J.W.: speaking honoraria, BY. G.T.: speaking and advisory board honoraria, BI, DSA, and BY. All other authors have nothing to report.
Figures

References
-
- Xian Y, O'Brien EC, Liang L, et al. Association of preceding antithrombotic treatment with acute ischemic stroke severity and in‐hospital outcomes among patients with atrial fibrillation. JAMA 2017;317:1057–1067. - PubMed
-
- Freedman B, Martinez C, Katholing A, Rietbrock S. Residual risk of stroke and death in anticoagulant‐treated patients with atrial fibrillation. JAMA Cardiol 2016;1:366–368. - PubMed
-
- Ruff CT, Giugliano RP, Braunwald E, et al. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: a meta‐analysis of randomised trials. Lancet 2014;383:955–962. - PubMed
-
- Cappellari M, Carletti M, Danese A, Bovi P. Early introduction of direct oral anticoagulants in cardioembolic stroke patients with non‐valvular atrial fibrillation. J Thromb Thrombolysis 2016;42:393–398. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
