

Travel-Associated and Locally Acquired Dengue Cases - United States, 2010-2017
- PMID: 32053577
- PMCID: PMC7017959
- DOI: 10.15585/mmwr.mm6906a1
Travel-Associated and Locally Acquired Dengue Cases - United States, 2010-2017
Abstract
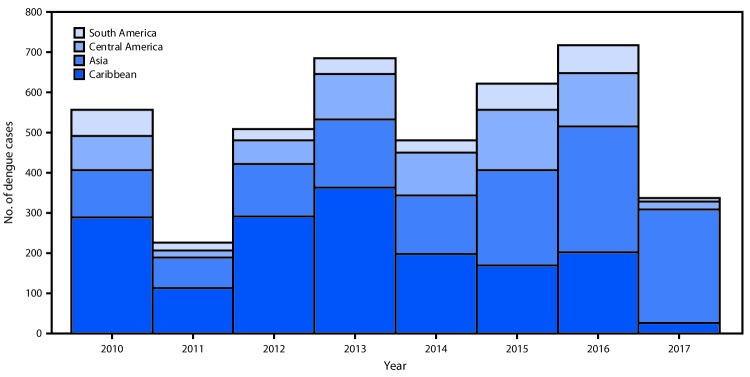
Dengue is a potentially fatal acute febrile illness caused by any of four mosquito-transmitted dengue viruses (DENV-1 to DENV-4) belonging to the family Flaviviridae and endemic throughout the tropics. Competent mosquito vectors of DENV are present in approximately one half of all U.S. counties. To describe epidemiologic trends in travel-associated and locally acquired dengue cases in the United States, CDC analyzed cases reported from the 50 states and District of Columbia to the national arboviral surveillance system (ArboNET). Cases are confirmed by detection of 1) virus RNA by reverse transcription-polymerase chain reaction (RT-PCR) in any body fluid or tissue, 2) DENV antigen in tissue by a validated assay, 3) DENV nonstructural protein 1 (NS1) antigen, or 4) immunoglobulin M (IgM) anti-DENV antibody if the patient did not report travel to an area with other circulating flaviviruses. When travel to an area with other flaviviruses was reported, IgM-positive cases were defined as probable. During 2010-2017, totals of 5,009 (93%) travel-associated and 378 (7%) locally acquired confirmed or probable dengue cases were reported to ArboNET. Cases were equally distributed between males and females, and median age was 41 years. Eighteen (three per 1,000) fatal cases were reported, all among travelers. Travelers should review country-specific recommendations (https://wwwnc.cdc.gov/travel/notices/watch/dengue-asia) for reducing their risk for DENV infection, including using insect repellent and staying in residences with air conditioning or screens on windows and doors.
Conflict of interest statement
All authors have completed and submitted the International Committee of Medical Journal Editors form for disclosure of potential conflicts of interest. No potential conflicts of interest were disclosed.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
