

A ten-year retrospective evaluation of acute flaccid myelitis at 5 pediatric centers in the United States, 2005-2014
- PMID: 32053652
- PMCID: PMC7018000
- DOI: 10.1371/journal.pone.0228671
A ten-year retrospective evaluation of acute flaccid myelitis at 5 pediatric centers in the United States, 2005-2014
Abstract
Background: Acute flaccid myelitis (AFM) is a severe illness similar to paralytic poliomyelitis. It is unclear how frequently AFM occurred in U.S. children after poliovirus elimination. In 2014, an AFM cluster was identified in Colorado, prompting passive US surveillance that yielded 120 AFM cases of unconfirmed etiology. Subsequently, increased reports were received in 2016 and 2018. To help inform investigations on causality of the recent AFM outbreaks, our objective was to determine how frequently AFM had occurred before 2014, and if 2014 cases had different characteristics.
Methods: We conducted a retrospective study covering 2005-2014 at 5 pediatric centers in 3 U.S. regions. Possible AFM cases aged ≤18 years were identified by searching discharge ICD-9 codes and spinal cord MRI reports (>37,000). Neuroradiologists assessed MR images, and medical charts were reviewed; possible cases were classified as AFM, not AFM, or indeterminate.
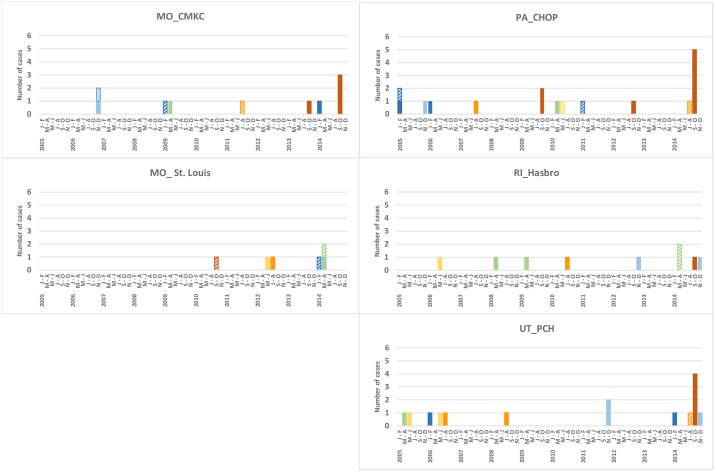
Results: At 5 sites combined, 26 AFM cases were identified from 2005-2013 (average annual number, 3 [2.4 cases/100,000 pediatric hospitalizations]) and 18 from 2014 (12.6 cases/100,000 hospitalizations; Poisson exact p<0.0001). A cluster of 13 cases was identified in September-October 2014 (temporal scan p = 0.0001). No other temporal or seasonal trend was observed. Compared with cases from January 2005-July 2014 (n = 29), cases from August-December 2014 (n = 15) were younger (p = 0.002), more frequently had a preceding respiratory/febrile illness (p = 0.03), had only upper extremities involved (p = 0.008), and had upper extremity monoplegia (p = 0.03). The cases had higher WBC counts in cerebrospinal fluid (p = 0.013).
Conclusion: Our data support emergence of AFM in 2014 in the United States, and those cases demonstrated distinctive features compared with preceding sporadic cases.
Conflict of interest statement
R.M. reports financial interests with Siemens Healthineers (travel, meals, lodging), Philips Healthcare (travel, meals, lodging) and Guerbet, LLC (consulting fees and travel expenses). S.H. receives salary support from the CDC for activities related to AFM surveillance. A.K. was employed by IHRC, Inc., a contracting agency to CDC. IHRC provided support in the form of salary for A.K. but did not have any additional role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript. The specific role of A.K. is articulated in the ‘author contributions’ section. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures



References
-
- Messacar K, Schreiner TL, Maloney JA, Wallace A, Ludke J, Oberste MS et al. A cluster of acute flaccid paralysis and cranial nerve dysfunction temporally associated with an outbreak of enterovirus D68 in children in Colorado, USA. Lancet. 2015;385(9978):1662–71. 10.1016/S0140-6736(14)62457-0 - DOI - PubMed
-
- Nathanson N. Epidemiologic aspects of poliomyelitis eradication. Rev Infect Dis. 1984. May-Jun;6 Suppl 2:S308–12 - PubMed
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
