

Determining the optimal time for liberation from renal replacement therapy in critically ill patients: a systematic review and meta-analysis (DOnE RRT)
- PMID: 32054522
- PMCID: PMC7020497
- DOI: 10.1186/s13054-020-2751-8
Determining the optimal time for liberation from renal replacement therapy in critically ill patients: a systematic review and meta-analysis (DOnE RRT)
Abstract
Introduction: Renal replacement therapy (RRT) is associated with high mortality and costs; however, no clinical guidelines currently provide specific recommendations for clinicians on when and how to stop RRT in recovering patients. Our objective was to systematically review the current evidence for clinical and biochemical parameters that can be used to predict successful discontinuation of RRT.
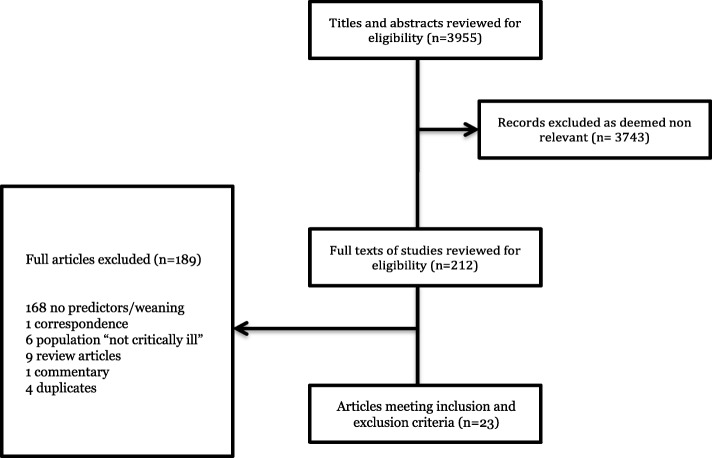
Methods: A systematic review and meta-analysis were performed with a peer-reviewed search strategy combining the themes of renal replacement therapy (IHD, CRRT, SLED), predictors of successful discontinuation or weaning (defined as an extended period of time free from further RRT), and patient outcomes. Major databases were searched and citations were screened using predefined criteria. Studied parameters were reported and, where possible, data was analyzed in the pooled analysis.
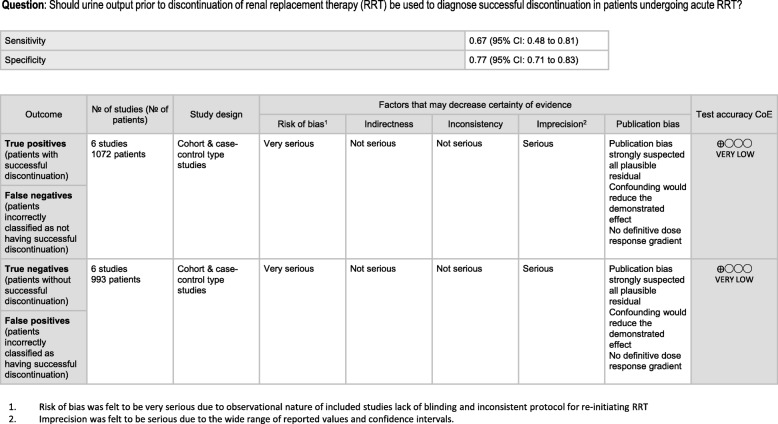
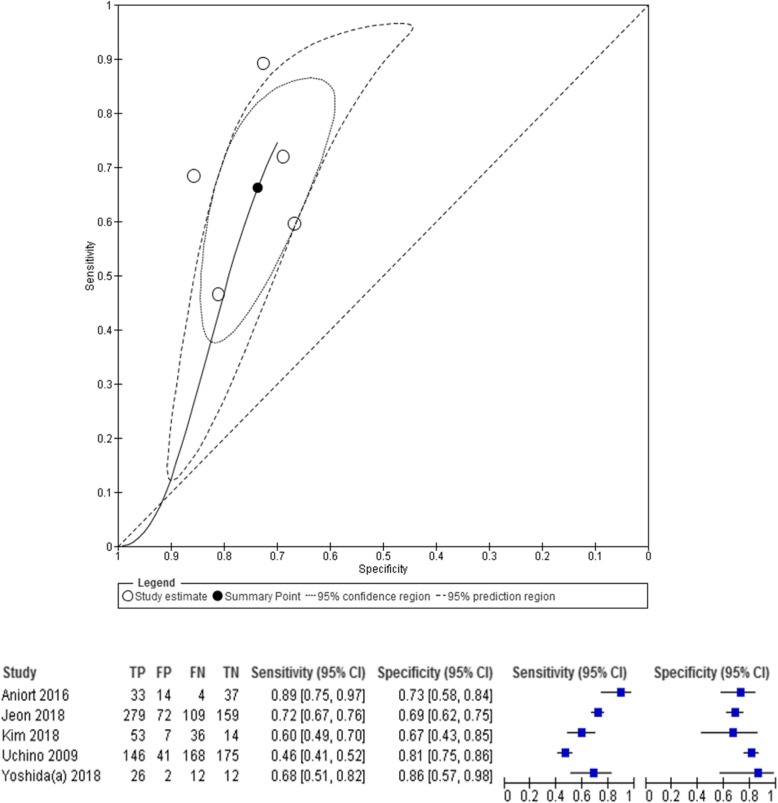
Results: Our search yielded 23 studies describing 16 variables for predicting the successful discontinuation of RRT. All studies were observational in nature. None were externally validated. Fourteen studies described conventional biochemical criteria used as surrogates of glomerular filtration rate (serum urea, serum creatinine, creatinine clearance, urine urea excretion, urine creatinine excretion). Thirteen studies described physiologic parameters such as urine output before and after cessation of RRT, and 13 studies reported on newer kidney biomarkers, such as serum cystatin C and serum neutrophil gelatinase-associated lipocalin (NGAL). Six studies reported sensitivity and specificity characteristics of multivariate models. Urine output prior to discontinuation of RRT was the most-studied variable, with nine studies reporting. Pooled analysis found a sensitivity of 66.2% (95% CI, 53.6-76.9%) and specificity of 73.6% (95% CI, 67.5-79.0%) for urine output to predict successful RRT discontinuation. Due to heterogeneity in the thresholds of urine output used across the studies, an optimal threshold value could not be determined.
Conclusions: Numerous variables have been described to predict successful discontinuation of RRT; however, available studies are limited by study design, variable heterogeneity, and lack of prospective validation. Urine output prior to discontinuation of RRT was the most commonly described and robust predictor. Further research should focus on the determination and validation of urine output thresholds, and the evaluation of additional clinical and biochemical parameters in multivariate models to enhance predictive accuracy.
Keywords: Acute kidney injury; Biomarkers; Creatinine; Intensive care unit; Prediction; Renal replacement therapy; Systematic review.
Conflict of interest statement
Dr. Bagshaw reports having received speaking fees and unrestricted funding support from Baxter Healthcare Corp.
Dr. Gibney reports having received speaking fees from Baxter Healthcare.
Dr. Silver reports having received speaking fees from Baxter Healthcare.
Figures
Comment in
-
Whether the GFR measured by renal scintigraphy under non-steady state conditions for critically ill patients with AKI can be used as a predictive parameter for clinical events.Crit Care. 2020 Apr 19;24(1):159. doi: 10.1186/s13054-020-02850-5. Crit Care. 2020. PMID: 32306989 Free PMC article. No abstract available.
References
-
- Nct: Standard vs. Accelerated Initiation of RRT in Acute Kidney Injury (STARRT-AKI: principal Trial). https://clinicaltrials.gov/show/nct02568722. 2015.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
