

To Infuse or Ingest in Human Laboratory Alcohol Research
- PMID: 32056250
- PMCID: PMC7166191
- DOI: 10.1111/acer.14305
To Infuse or Ingest in Human Laboratory Alcohol Research
Abstract
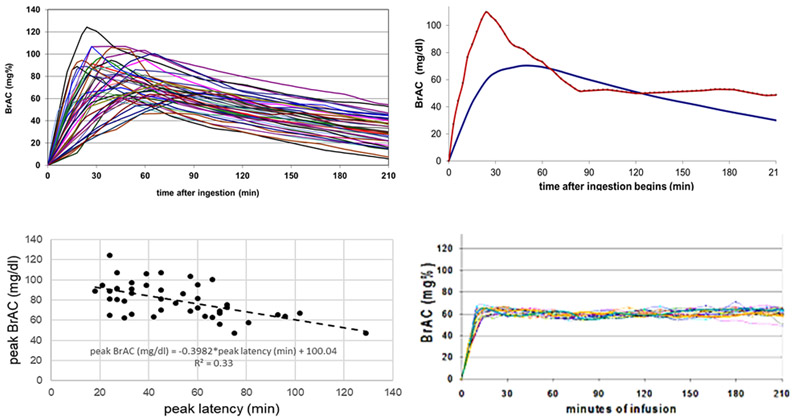
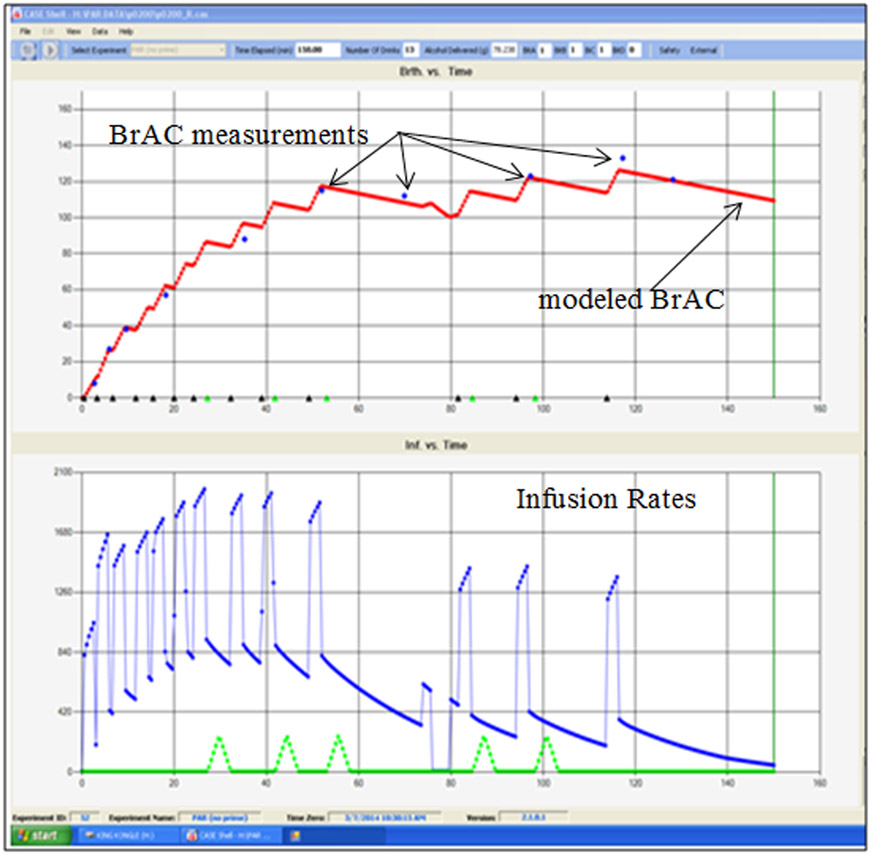
Human alcohol laboratory studies use two routes of alcohol administration: ingestion and infusion. The goal of this paper was to compare and contrast these alcohol administration methods. The work summarized in this report was the basis of a 2019 Research Society on Alcoholism Roundtable, "To Ingest or Infuse: A Comparison of Oral and Intravenous Alcohol Administration Methods for Human Alcohol Laboratory Designs." We review the methodological approaches of each and highlight strengths and weaknesses pertaining to different research questions. We summarize methodological considerations to aid researchers in choosing the most appropriate method for their inquiry, considering exposure variability, alcohol expectancy effects, safety, bandwidth, technical skills, documentation of alcohol exposure, experimental variety, ecological validity, and cost. Ingestion of alcohol remains a common and often a preferable, methodological practice in alcohol research. Nonetheless, the main problem with ingestion is that even the most careful calculation of dose and control of dosing procedures yields substantial and uncontrollable variability in the participants' brain exposures to alcohol. Infusion methodologies provide precise exposure control but are technically complex and may be limited in ecological validity. We suggest that alcohol ingestion research may not be the same thing as alcohol exposure research; investigators should be aware of the advantages and disadvantages that the choice between ingestion and infusion of alcohol invokes.
Keywords: Alcohol Experiments; Human Laboratory Research; Intravenous Alcohol Infusion; Oral Alcohol Ingestion.
© 2020 by the Research Society on Alcoholism.
Figures
References
-
- Aalto S, Ingman K, Alakurtti K, Kaasinen V, Virkkala J, Någren K, Rinne JO, & Scheinin H (2015). Intravenous ethanol increases dopamine release in the ventral striatum in humans: PET study using bolus-plus-infusion administration of [11 C]raclopride. Journal of Perinatology, 35(3), 424–431. 10.1038/jcbfm.2014.209 - DOI - PMC - PubMed
-
- Blekher T, Ramchandani V. a, Flury L, Foroud T, Kareken D, Yee RD, Li TK, & O’Connor S (2002). Saccadic eye movements are associated with a family history of alcoholism at baseline and after exposure to alcohol. Alcoholism, Clinical and Experimental Research, 26(10), 1568–1573. 10.1097/01.ALC.0000033121.05006.EF - DOI - PubMed
-
- Bujarski S, David Jentsch J, Roche DJO, Ramchandani VA, Miotto K, & Ray LA (2018). Differences in the subjective and motivational properties of alcohol across alcohol use severity: Application of a novel translational human laboratory paradigm. Neuropsychopharmacology, 43(9), 1891–1899. 10.1038/s41386-018-0086-9 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
