

Sepsis Among Medicare Beneficiaries: 2. The Trajectories of Sepsis, 2012-2018
- PMID: 32058367
- PMCID: PMC7017944
- DOI: 10.1097/CCM.0000000000004226
Sepsis Among Medicare Beneficiaries: 2. The Trajectories of Sepsis, 2012-2018
Abstract
Objectives: To distinguish characteristics of Medicare beneficiaries who will have an acute inpatient admission for sepsis from those who have an inpatient admission without sepsis, and to describe their further trajectories during and subsequent to those inpatient admissions.
Design: Analysis of paid Medicare claims via the Centers for Medicare and Medicaid Services DataLink Project.
Setting: All U.S. acute care hospitals, excepting federal hospitals (Veterans Administration and Defense Health Agency).
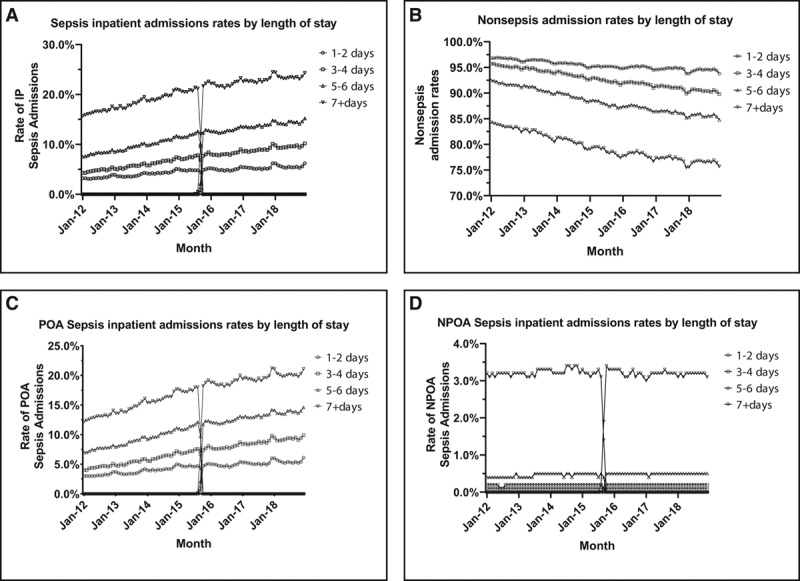
Patients: Medicare beneficiaries, 2012-2018, with an inpatient hospital admission including one or more explicit sepsis codes.
Interventions: None.
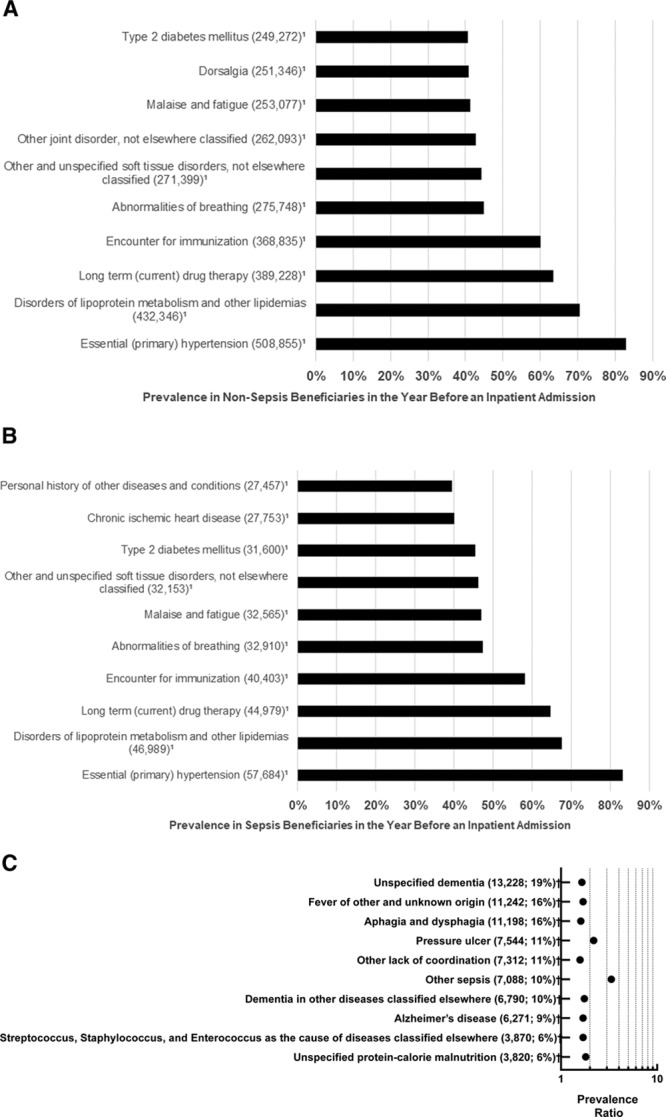
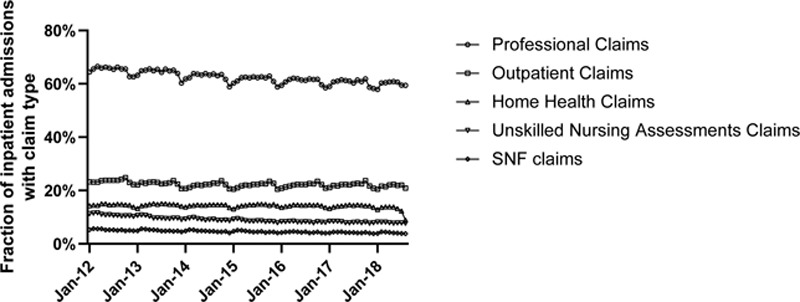
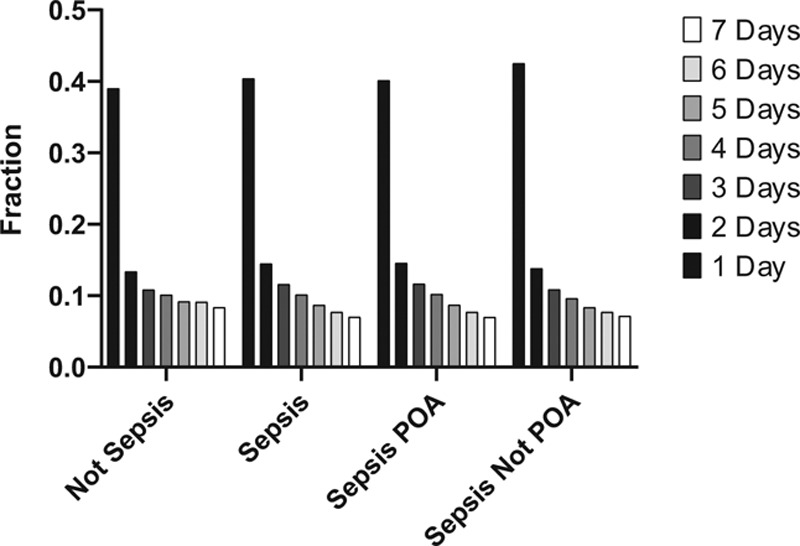
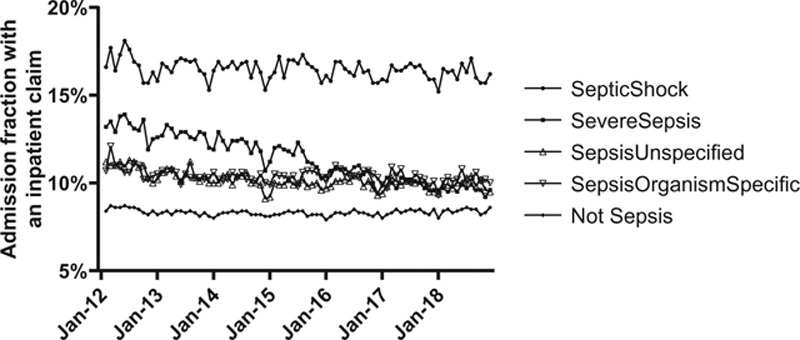
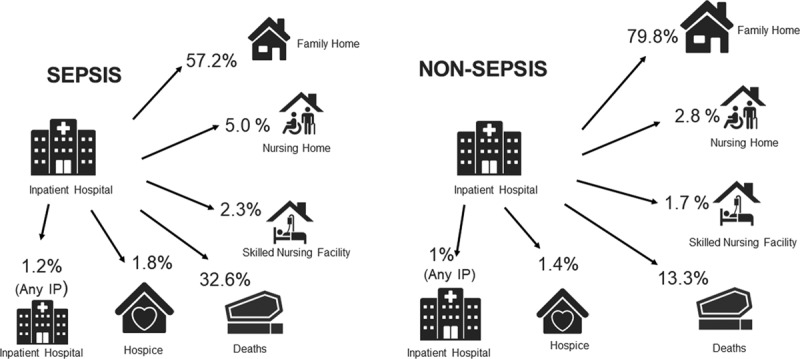
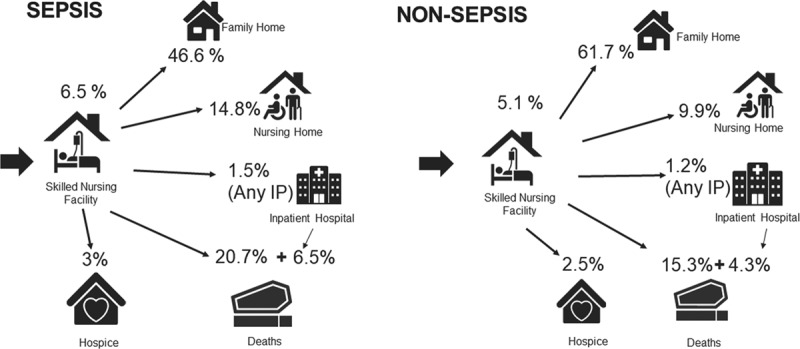
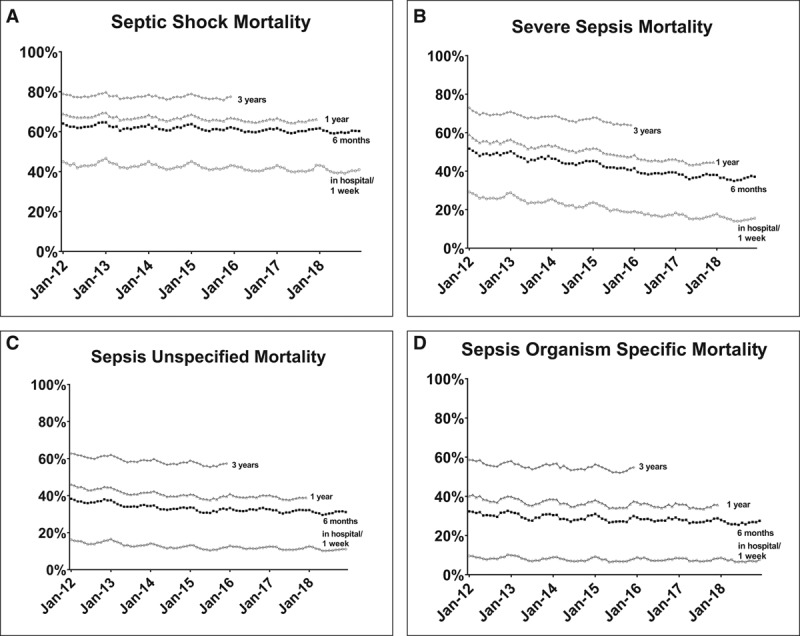
Measurements and main results: Prevalent diagnoses in the year prior to the inpatient admission; healthcare contacts in the week prior to the inpatient admission; discharges, transfers, readmissions, and deaths (trajectories) for 6 months following discharge from the inpatient admission. Beneficiaries with no sepsis inpatient hospital admission for a year prior to an index hospital admission for sepsis were nearly indistinguishable by accumulated diagnostic codes from beneficiaries who had an index hospital admission without sepsis. Although the timing of healthcare services in the week prior to inpatient hospital admission was similar among beneficiaries who would be admitted for sepsis versus those whose inpatient admission did not include a sepsis code, the setting differed: beneficiaries destined for a sepsis admission were more likely to have received skilled nursing or unskilled nursing (e.g., nursing aide for activities of daily living) care. In contrast, comparing beneficiaries who had been free of any inpatient admission for an entire year and then required an inpatient admission, acute inpatient stays that included a sepsis code led to more than three times as many deaths within 1 week of discharge, with more admissions to skilled nursing facilities and fewer discharges to home. Comparing all beneficiaries who were admitted to a skilled nursing facility after an inpatient hospital admission, those who had sepsis coded during the index admission were more likely to die in the skilled nursing facility; more likely to be readmitted to an acute inpatient hospital and subsequently die in that setting; or if they survive to discharge from the skilled nursing facility, they are more likely to go next to a custodial nursing home.
Conclusions: Although Medicare beneficiaries destined for an inpatient hospital admission with a sepsis code are nearly indistinguishable by other diagnostic codes from those whose admissions will not have a sepsis code, their healthcare trajectories following the admission are worse. This suggests that an inpatient stay that included a sepsis code not only identifies beneficiaries who were less resilient to infection but also signals increased risk for worsening health, for mortality, and for increased use of advanced healthcare services during and postdischarge along with an increased likelihood of an inpatient hospital readmission.
Figures
Comment in
-
Identifying the Burden of Sepsis With Big Data.Crit Care Med. 2020 Mar;48(3):422-423. doi: 10.1097/CCM.0000000000004229. Crit Care Med. 2020. PMID: 32058377 No abstract available.
References
-
- Rothman M, Levy M, Dellinger RP, et al. Sepsis as 2 problems: Identifying sepsis at admission and predicting onset in the hospital using an electronic medical record-based acuity score. J Crit Care 2017; 38:237–244 - PubMed
-
- Maley JH, Mikkelsen ME. Short-term gains with long-term consequences: The evolving story of sepsis survivorship. Clin Chest Med 2016; 37:367–380 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
