

Critical Illness Factors Associated With Long-Term Mortality and Health-Related Quality of Life Morbidity Following Community-Acquired Pediatric Septic Shock
- PMID: 32058369
- PMCID: PMC7089387
- DOI: 10.1097/CCM.0000000000004122
Critical Illness Factors Associated With Long-Term Mortality and Health-Related Quality of Life Morbidity Following Community-Acquired Pediatric Septic Shock
Abstract
Objectives: A companion article reports the trajectory of long-term mortality and significant health-related quality of life disability among children encountering septic shock. In this article, the investigators examine critical illness factors associated with these adverse outcomes.
Design: Prospective, cohort-outcome study, conducted 2013-2017.
Setting: Twelve United States academic PICUs.
Patients: Critically ill children, 1 month to 18 years, with community-acquired septic shock requiring vasoactive-inotropic support.
Interventions: Illness severity, organ dysfunction, and resource utilization data were collected during PICU admission. Change from baseline health-related quality of life at the month 3 follow-up was assessed by parent proxy-report employing the Pediatric Quality of Life Inventory or the Stein-Jessop Functional Status Scale.
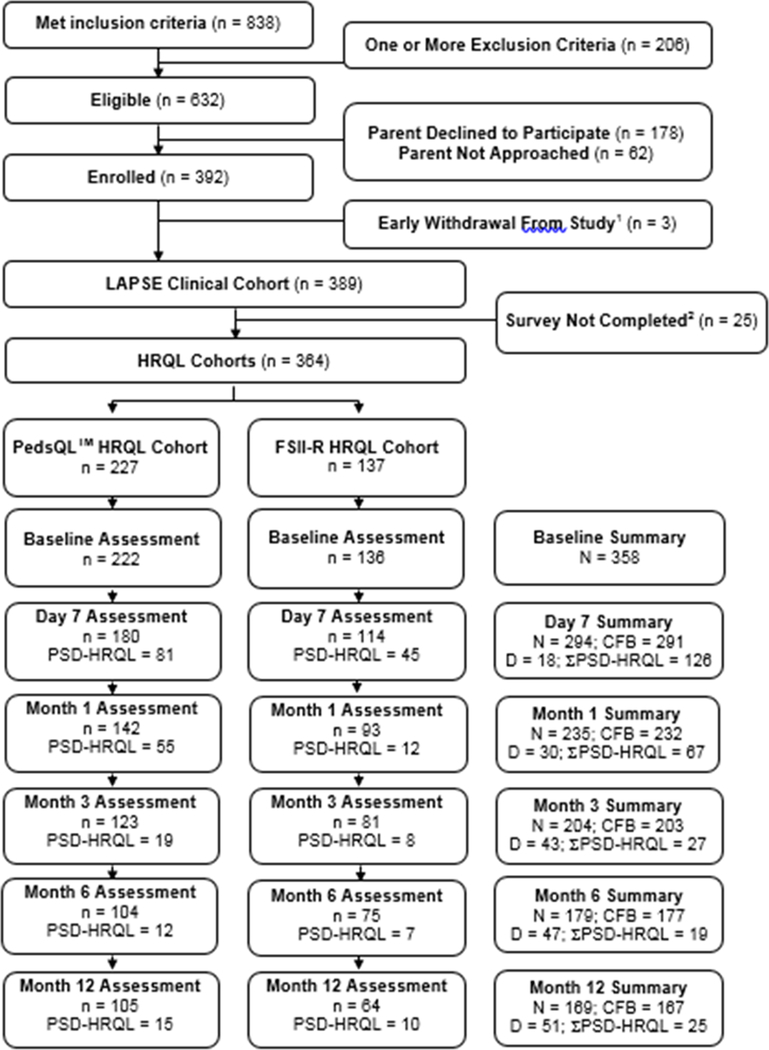
Measurements and main results: In univariable modeling, critical illness variables associated with death and/or persistent, serious health-related quality of life deterioration were candidates for multivariable modeling using Bayesian information criterion. The most clinically relevant multivariable models were selected among models with near-optimal statistical fit. Three months following septic shock, 346 of 389 subjects (88.9%) were alive and 43 of 389 had died (11.1%); 203 of 389 (52.2%) had completed paired health-related quality of life surveys. Pediatric Risk of Mortality, cumulative Pediatric Logistic Organ Dysfunction scores, PICU and hospital durations of stay, maximum and cumulative vasoactive-inotropic scores, duration of mechanical ventilation, need for renal replacement therapy, extracorporeal life support or cardiopulmonary resuscitation, and appearance of pathologic neurologic signs were associated with adverse outcomes in univariable models. In multivariable regression analysis (odds ratio [95% CI]), summation of daily Pediatric Logistic Organ Dysfunction scores, 1.01/per point (1.01-1.02), p < 0.001; highest vasoactive-inotropic score, 1.02/per point (1.00-1.04), p = 0.003; and any acute pathologic neurologic sign/event, 5.04 (2.15-12.01), p < 0.001 were independently associated with death or persistent, serious deterioration of health-related quality of life at month 3.
Conclusions and relevance: Biologically plausible factors related to sepsis-associated critical illness organ dysfunction and its treatment were associated with poor outcomes at month 3 follow-up among children encountering septic shock.
Conflict of interest statement
The authors have disclosed that they do not have any potential conflicts of interest.
Figures
Comment in
-
Septic Shock in Children: When Should Prevention Start and Treatment End?Crit Care Med. 2020 Mar;48(3):426-428. doi: 10.1097/CCM.0000000000004230. Crit Care Med. 2020. PMID: 32058379 No abstract available.
References
-
- Hartman ME, Linde-Zwirble WT, Angus DC, et al. : Trends in the epidemiology of pediatric severe sepsis. Pediatr Crit Care Med 2013; 14:686–693 - PubMed
-
- Ruth A, McCracken CE, Fortenberry JD, et al. : Pediatric severe sepsis: current trends and outcomes from the Pediatric Health Information Systems database. Pediatr Crit Care Med 2014; 15:828–838 - PubMed
-
- Simon DW, Clark RS, Watson RR: No pain, no gain in pediatric sepsis?. Pediatr Crit Care Med 2014; 15:264–266 - PubMed
Publication types
MeSH terms
Grants and funding
- U10 HD063108/HD/NICHD NIH HHS/United States
- U10 HD050012/HD/NICHD NIH HHS/United States
- UG1 HD049983/HD/NICHD NIH HHS/United States
- UG1 HD050096/HD/NICHD NIH HHS/United States
- U10 HD049981/HD/NICHD NIH HHS/United States
- U10 HD050096/HD/NICHD NIH HHS/United States
- U10 HD049983/HD/NICHD NIH HHS/United States
- U10 HD063106/HD/NICHD NIH HHS/United States
- UG1 HD063108/HD/NICHD NIH HHS/United States
- RL1 HD107773/HD/NICHD NIH HHS/United States
- R01 HD073362/HD/NICHD NIH HHS/United States
- UG1 HD083171/HD/NICHD NIH HHS/United States
- U10 HD063114/HD/NICHD NIH HHS/United States
- U01 HD049934/HD/NICHD NIH HHS/United States
- UG1 HD049981/HD/NICHD NIH HHS/United States
- UG1 HD083170/HD/NICHD NIH HHS/United States
- UG1 HD083166/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
