

Trajectory of Mortality and Health-Related Quality of Life Morbidity Following Community-Acquired Pediatric Septic Shock
- PMID: 32058370
- PMCID: PMC7164680
- DOI: 10.1097/CCM.0000000000004123
Trajectory of Mortality and Health-Related Quality of Life Morbidity Following Community-Acquired Pediatric Septic Shock
Abstract
Objectives: In-hospital pediatric sepsis mortality has decreased substantially, but long-term mortality and morbidity among children initially surviving sepsis, is unknown. Accordingly, the Life After Pediatric Sepsis Evaluation investigation was conducted to describe the trajectory of mortality and health-related quality of life morbidity for children encountering community-acquired septic shock.
Design: Prospective, cohort-outcome study, conducted 2013-2017.
Setting: Twelve academic PICUs in the United States.
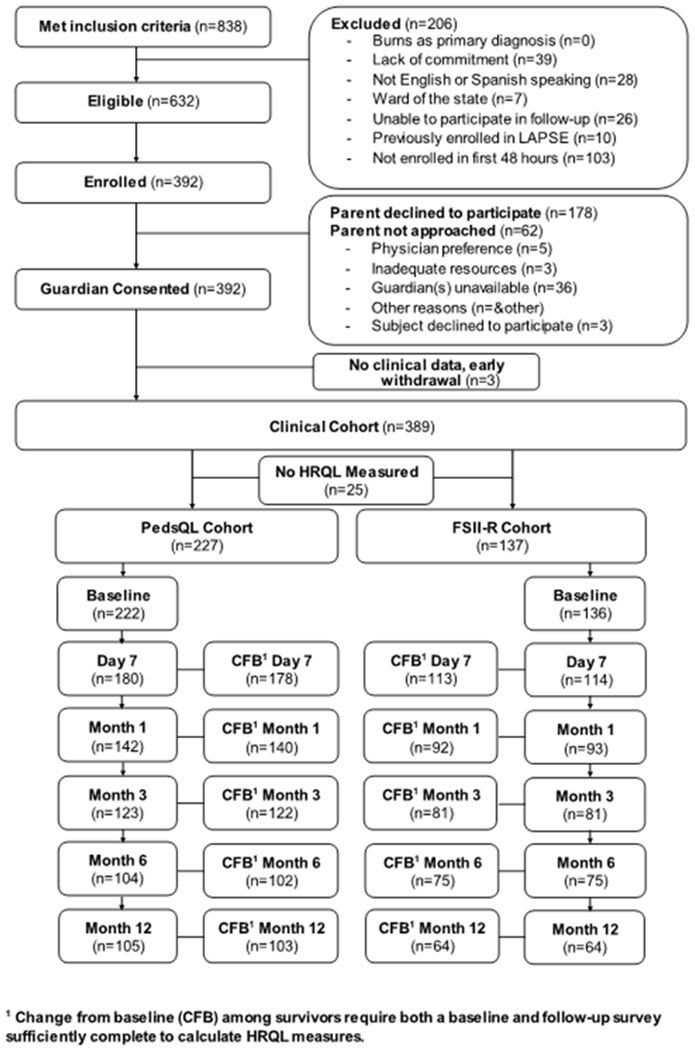
Patients: Critically ill children, 1 month to 18 years, with community-acquired septic shock requiring vasoactive-inotropic support.
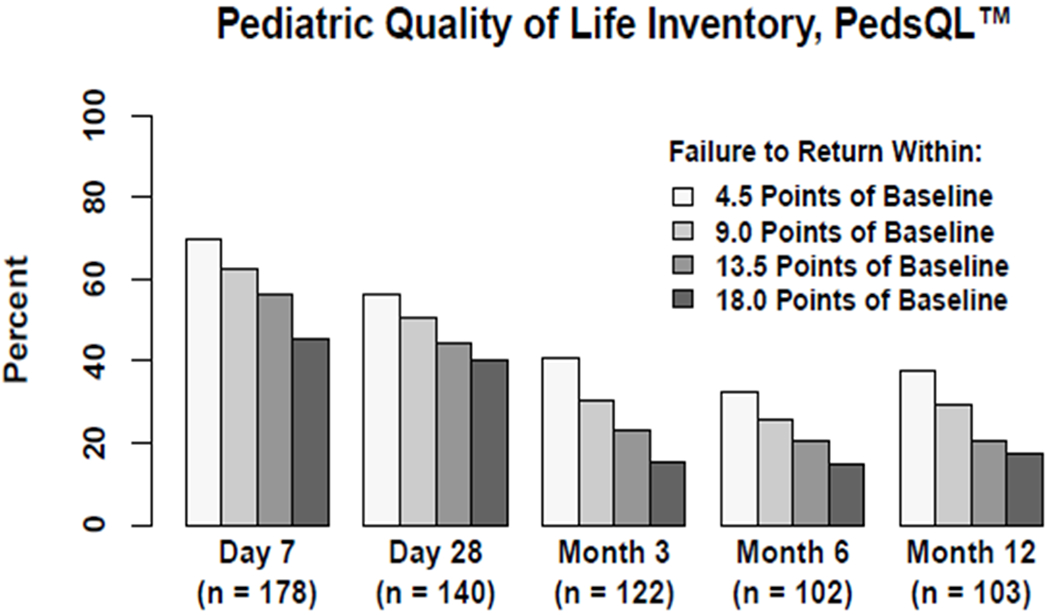
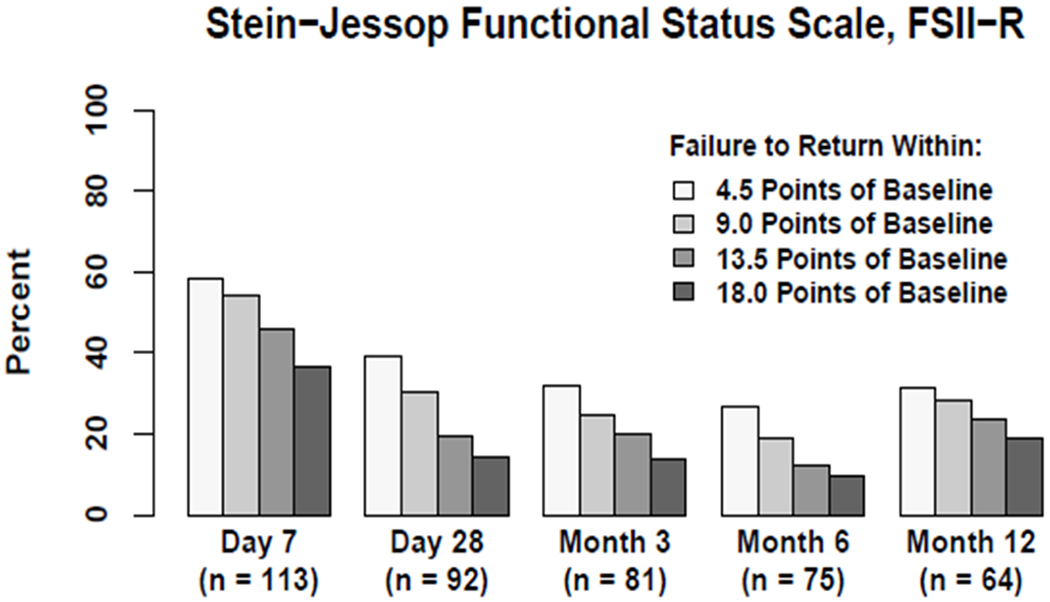
Interventions: Demographic, infection, illness severity, organ dysfunction, and resource utilization data were collected daily during PICU admission. Serial parent proxy-report health-related quality of life assessments were obtained at baseline, 7 days, and 1, 3, 6, and 12 months following PICU admission utilizing the Pediatric Quality of Life Inventory or Stein-Jessop Functional Status Scale.
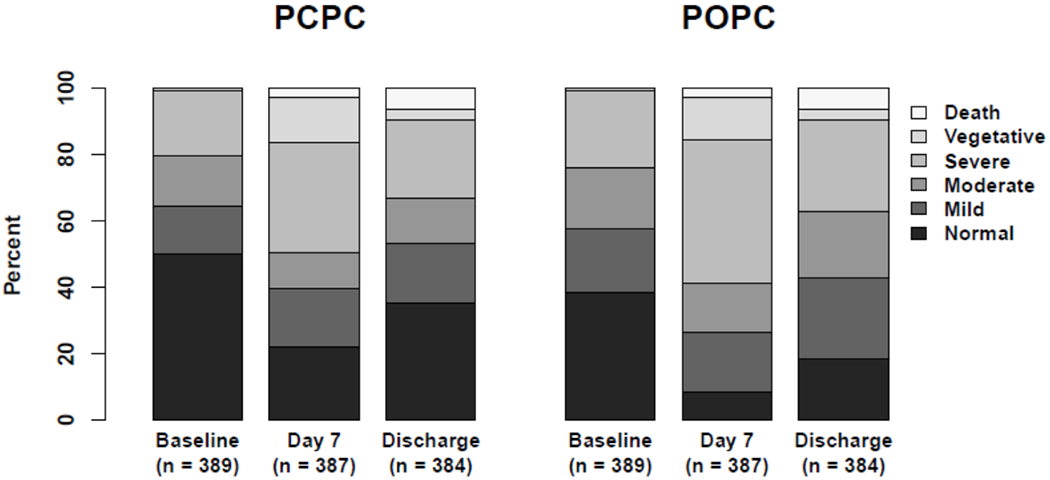
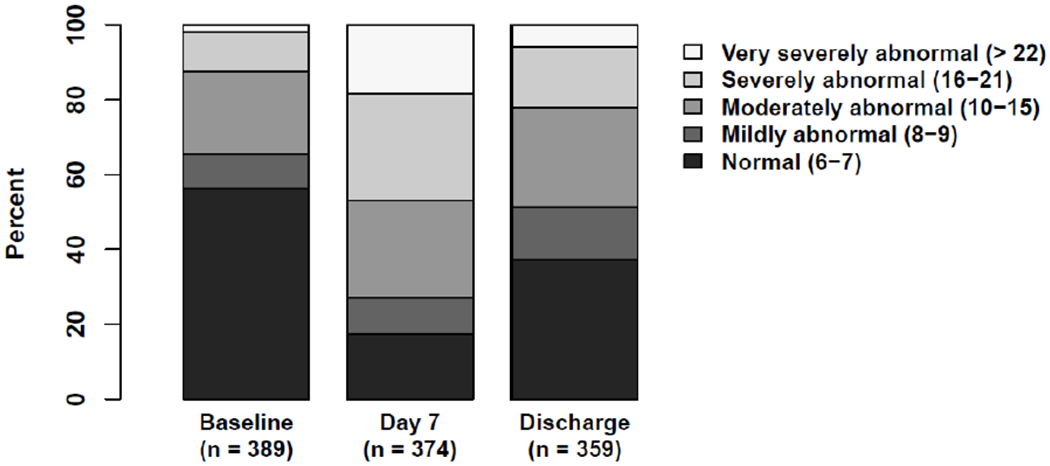
Measurements and main results: Among 389 children enrolled, mean age was 7.4 ± 5.8 years; 46% were female; 18% were immunocompromised; and 51% demonstrated chronic comorbidities. Baseline Pediatric Overall Performance Category was normal in 38%. Median (Q1-Q3) Pediatric Risk of Mortality and Pediatric Logistic Organ Dysfunction scores at PICU admission were 11.0 (6.0-17.0) and 9.0 (6.0-11.0); durations of vasoactive-inotropic and mechanical ventilation support were 3.0 days (2.0-6.0 d) and 8.0 days (5.0-14.0 d); and durations of PICU and hospital stay were 9.4 days (5.6-15.4 d) and 15.7 days (9.2-26.0 d). At 1, 3, 6, and 12 months following PICU admission for the septic shock event, 8%, 11%, 12%, and 13% of patients had died, while 50%, 37%, 30%, and 35% of surviving patients had not regained their baseline health-related quality of life.
Conclusions: This investigation provides the first longitudinal description of long-term mortality and clinically relevant, health-related quality of life morbidity among children encountering community-acquired septic shock. Although in-hospital mortality was 9%, 35% of survivors demonstrated significant, health-related quality of life deterioration from baseline that persisted at least 1 year following hospitalization for septic shock.
Figures
Comment in
-
Septic Shock in Children: When Should Prevention Start and Treatment End?Crit Care Med. 2020 Mar;48(3):426-428. doi: 10.1097/CCM.0000000000004230. Crit Care Med. 2020. PMID: 32058379 No abstract available.
References
-
- Hartman ME, Linde-Zwirble WT, Angus DC, et al. : Trends in the epidemiology of pediatric severe sepsis. Pediatr Crit Care Med 2013; 14:686–693 - PubMed
-
- Ruth A, McCracken CE, Fortenberry JD, et al. : Pediatric severe sepsis: current trends and outcomes from the Pediatric Health Information Systems database. Pediatr Crit Care Med 2014; 15:828–838 - PubMed
Publication types
MeSH terms
Grants and funding
- U10 HD050012/HD/NICHD NIH HHS/United States
- UG1 HD049983/HD/NICHD NIH HHS/United States
- UG1 HD050096/HD/NICHD NIH HHS/United States
- U10 HD063106/HD/NICHD NIH HHS/United States
- UG1 HD063108/HD/NICHD NIH HHS/United States
- RL1 HD107773/HD/NICHD NIH HHS/United States
- R01 HD073362/HD/NICHD NIH HHS/United States
- UG1 HD083171/HD/NICHD NIH HHS/United States
- U01 HD049934/HD/NICHD NIH HHS/United States
- UG1 HD049981/HD/NICHD NIH HHS/United States
- UG1 HD083170/HD/NICHD NIH HHS/United States
- UG1 HD083166/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
