

Systemic Endothelial Activation Is Associated With Early Acute Respiratory Distress Syndrome in Children With Extrapulmonary Sepsis
- PMID: 32058372
- PMCID: PMC8749338
- DOI: 10.1097/CCM.0000000000004091
Systemic Endothelial Activation Is Associated With Early Acute Respiratory Distress Syndrome in Children With Extrapulmonary Sepsis
Abstract
Objectives: Systemic endothelial activation may contribute to sepsis-associated organ injury, including acute respiratory distress syndrome. We hypothesized that children with extrapulmonary sepsis with versus without acute respiratory distress syndrome would have plasma biomarkers indicative of increased endothelial activation and that persistent biomarker changes would be associated with poor outcome.
Design: Observational cohort.
Setting: Academic PICU.
Patients: Patients less than 18 years old with sepsis from extrapulmonary infection with (n = 46) or without (n = 54) acute respiratory distress syndrome and noninfected controls (n = 19).
Interventions: None.
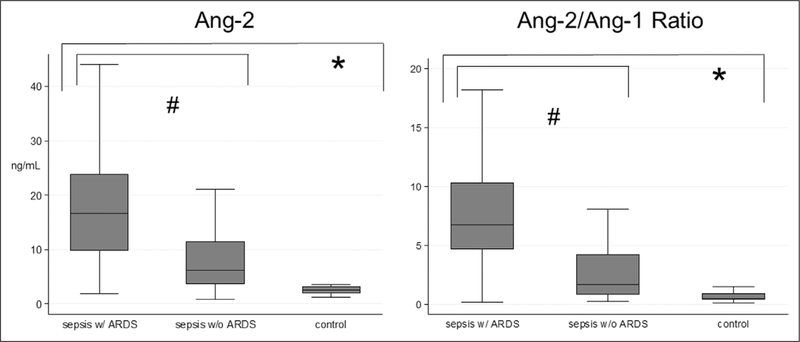
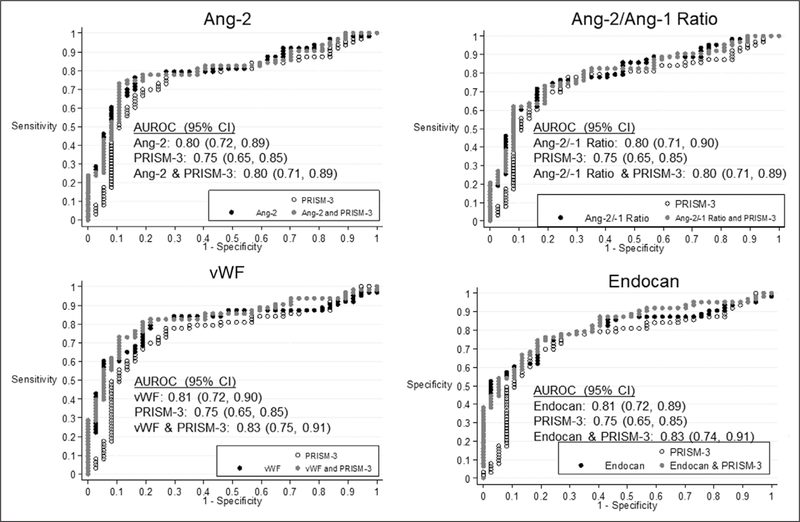
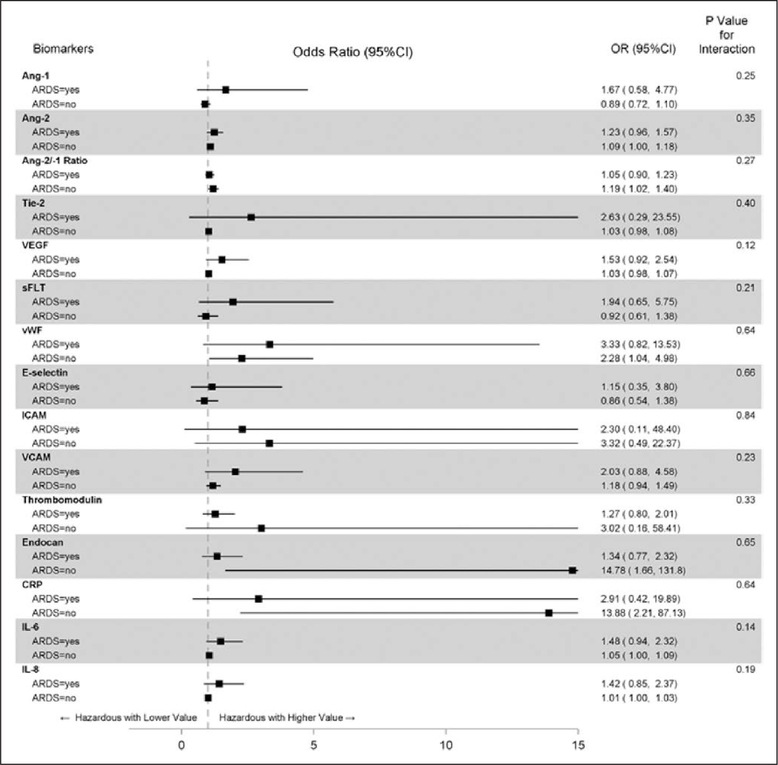
Measurements and main results: Endothelial (angiopoietin-1, angiopoietin-2, tyrosine kinase with immunoglobulin-like loop epidermal growth factor homology domain 2, vascular endothelial growth factor, soluble fms-like tyrosine kinase, von Willebrand factor, E-selectin, intercellular adhesion molecule, vascular cell adhesion molecule, thrombomodulin) and inflammatory biomarkers (C-reactive protein, interleukin-6, and interleukin-8) were measured from peripheral plasma collected within 3 days (time 1) of sepsis recognition and at 3-6 days (time 2) and 7-14 days (time 3). Time 1 biomarkers and longitudinal measurements were compared for sepsis patients with versus without acute respiratory distress syndrome and in relation to complicated course, defined as greater than or equal to two organ dysfunctions at day 7 or death by day 28. Angiopoietin-2, angiopoietin-2/angiopoietin-1 ratio, tyrosine kinase with immunoglobulin-like loop epidermal growth factor homology domain 2, vascular endothelial growth factor, von Willebrand factor, E-selectin, intercellular adhesion molecule, vascular cell adhesion molecule, thrombomodulin, endocan, C-reactive protein, interleukin-6, and interleukin-8 were different between sepsis and noninfected control patients at time 1. Among patients with sepsis, those with acute respiratory distress syndrome had higher angiopoietin-2/angiopoietin-1 ratio, vascular endothelial growth factor, vascular cell adhesion molecule, thrombomodulin, endocan, interleukin-6, and interleukin-8 than those without acute respiratory distress syndrome (all p < 0.003). Angiopoietin-2 and angiopoietin-2/angiopoietin-1 ratio remained higher in sepsis with versus without acute respiratory distress syndrome after multivariable analyses. Time 1 measures of angiopoietin-2, angiopoietin-2/-1 ratio, von Willebrand factor, and endocan were indicative of complicated course in all sepsis patients (all area under the receiver operating curve ≥ 0.80). In sepsis without acute respiratory distress syndrome, soluble fms-like tyrosine kinase decreased more quickly and von Willebrand factor and thrombomodulin decreased more slowly in those with complicated course.
Conclusions: Children with extrapulmonary sepsis with acute respiratory distress syndrome had plasma biomarkers indicative of greater systemic endothelial activation than those without acute respiratory distress syndrome. Several endothelial biomarkers measured near sepsis recognition were associated with complicated course, whereas longitudinal biomarker changes yielded prognostic information only in those without sepsis-associated acute respiratory distress syndrome.
Figures
Comment in
-
Potential Value of Biomarker Signatures in Sepsis and Acute Respiratory Distress Syndrome in Children and Adults.Crit Care Med. 2020 Mar;48(3):428-430. doi: 10.1097/CCM.0000000000004169. Crit Care Med. 2020. PMID: 32058380 No abstract available.
References
-
- Flori HR, Glidden DV, Rutherford GW, et al. : Pediatric acute lung injury: prospective evaluation of risk factors associated with mortality. Am J Respir Crit Care Med 2005; 171:995–1001 - PubMed
-
- Weiss SL, Fitzgerald JC, Pappachan J, et al. ; Sepsis Prevalence, Outcomes, and Therapies (SPROUT) Study Investigators and Pediatric Acute Lung Injury and Sepsis Investigators (PALISI) Network: Global epidemiology of pediatric severe sepsis: The sepsis prevalence, outcomes, and therapies study. Am J Respir Crit Care Med 2015; 191:1147–1157 - PMC - PubMed
-
- López-Fernández Y, Azagra AM, de la Oliva P, et al. ; Pediatric Acute Lung Injury Epidemiology and Natural History (PED-ALIEN) Network: Pediatric acute lung injury epidemiology and natural history study: Incidence and outcome of the acute respiratory distress syndrome in children. Crit Care Med 2012; 40:3238–3245 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
