

Acute kidney injury in heart failure: a population study
- PMID: 32059081
- PMCID: PMC7160477
- DOI: 10.1002/ehf2.12595
Acute kidney injury in heart failure: a population study
Abstract
Aims: The objective of the present study is to assess the prognostic value of acute kidney injury (AKI) in the evolution of patients with heart failure (HF) using real-world data.
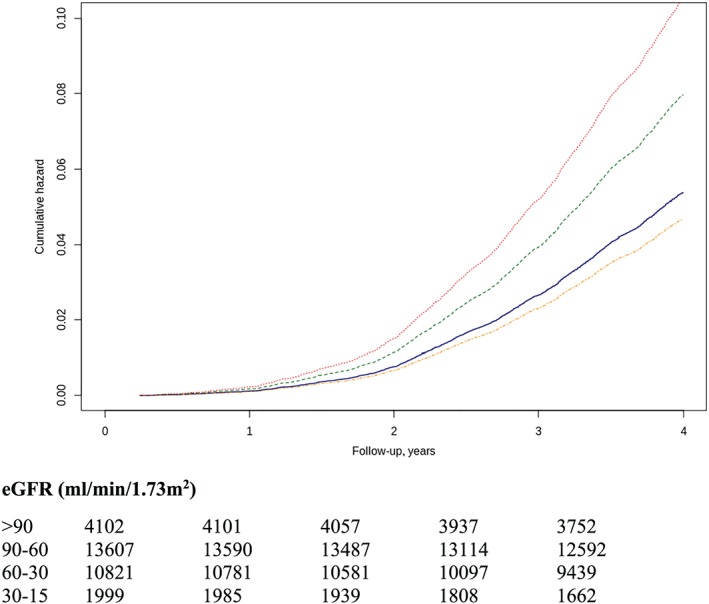
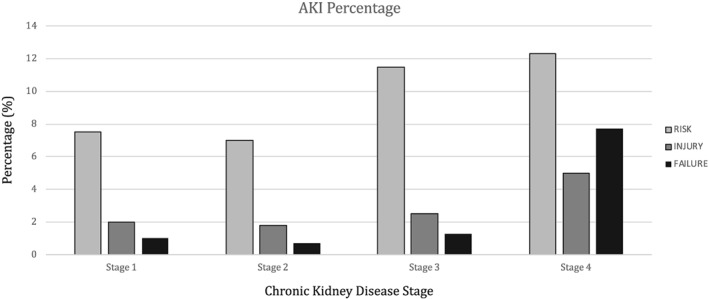
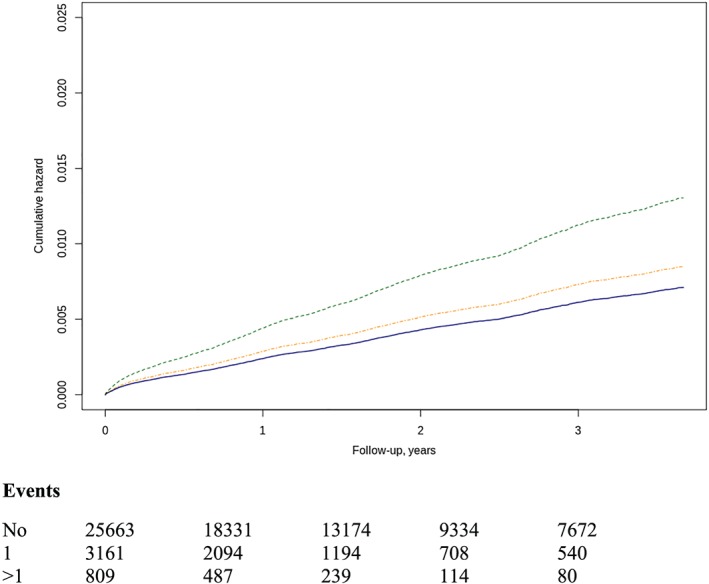
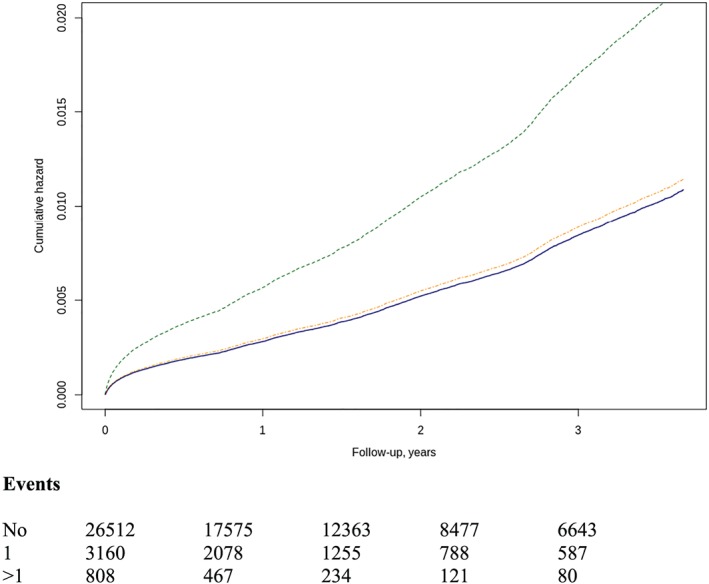
Methods and results: Patients with a diagnosis of HF and with serial measurements of renal function collected throughout the study period were included. Estimated glomerular filtration rate (GFR) was calculated with the CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration). AKI was defined when a sudden drop in creatinine with posterior recovery was recorded. According to the Risk, Injury, Failure, Loss, and End-Stage Renal Disease (RIFLE) scale, AKI severity was graded in three categories: risk [1.5-fold increase in serum creatinine (sCr)], injury (2.0-fold increase in sCr), and failure (3.0-fold increase in sCr or sCr > 4.0 mg/dL). AKI incidence and risk of hospitalization and mortality after the first episode were calculated by adjusting for potential confounders. A total of 30 529 patients with HF were included. During an average follow-up of 3.2 years, 5294 AKI episodes in 3970 patients (13.0%) and incidence of 3.3/100 HF patients/year were recorded. One episode was observed in 3161 (10.4%), two in 537 (1.8%), and three or more in 272 (0.9%). They were more frequent in women with diabetes and hypertension. The incidence increases across the GFR levels (Stages 1 to 4: risk 7.6%, 6.8%, 11.3%, and 12.5%; injury 2.1%, 2.0%, 3.3%, and 5.5%; and failure 0.9%, 0.6%. 1.4%, and 8.0%). A total of 3817 patients with acute HF admission were recorded during the follow-up, with incidence of 38.4/100 HF patients/year, 3101 (81.2%) patients without AKI, 545 (14.3%) patients with one episode, and 171 (4.5%) patients with two or more. The number of AKI episodes [one hazard ratio (HR) 1.05 (0.98-1.13); two or more HR 2.01 (1.79-2.25)] and severity [risk HR 1.05 (0.97-1.04); injury HR 1.41 (1.24-1.60); and failure HR 1.90 (1.64-2.20)] increases the risk of hospitalization. A total of 10 560 deaths were recorded, with incidence of 9.3/100 HF patients/year, 8951 (33.7%) of subjects without AKI episodes, 1180 (11.17%) of subjects with one episode, and 429 (4.06%) with two or more episodes. The number of episodes [one HR 1.05 (0.98-1.13); two or more HR 2.01 (1.79-2.25)] and severity [risk 1.05 confidence interval (CI) (0.97-1.14), injury 1.41 (CI 1.24-1.60), and failure 1.90 (CI 1.64-2.20)] increases mortality risk.
Conclusions: The study demonstrated the worse prognostic value of sudden renal function decline in HF patients and pointed to those with more future risk who require review of treatment and closer follow-up.
Keywords: Acute kidney injury; Heart failure; Renal function; Risk of hospitalization; Risk of mortality.
© 2020 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of the European Society of Cardiology.
Conflict of interest statement
None declared.
Figures
References
-
- Schefold JC, Filippatos G, Hasenfuss G, Anker SD, von Haehling S. Heart failure and kidney dysfunction: epidemiology, mechanisms and management. Nat Rev Nephrol 2016; 12: 610–623. - PubMed
-
- Smith GL, Lichtman JH, Bracken MB, Shlipak MG, Phillips CO, DiCapua P, Krumholz HM. Renal impairment and outcomes in heart failure: systematic review and meta‐analysis. J Am Coll Cardiol 2006; 47: 1987–1996. - PubMed
-
- Takagi A, Iwama Y, Yamada A, Aihara K, Daida H. Estimated glomerular filtration rate is an independent predictor for mortality of patients with acute heart failure. J Cardiol 2010; 55: 317–321. - PubMed
-
- Heywood JT, Fonarow GC, Costanzo MR, Mathur VS, Wigneswaran JR, Wynne J. High prevalence of renal dysfunction and its impact on outcome in 118,465 patients hospitalized with acute decompensated heart failure: a report from the ADHERE database. J Card Fail 2007; 13: 422–430. - PubMed
-
- Gansevoort RT, Correa‐Rotter R, Hemmelgarn BR, Jafar TH, Heerspink HJ, Mann JF, Matsushita K, Wen CP. Chronic kidney disease and cardiovascular risk: epidemiology, mechanisms, and prevention. Lancet 2013; 382: 339–352. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous