

Regional Variation in the Management and Outcomes of Acute Myocardial Infarction With Cardiogenic Shock in the United States
- PMID: 32059628
- PMCID: PMC7027926
- DOI: 10.1161/CIRCHEARTFAILURE.119.006661
Regional Variation in the Management and Outcomes of Acute Myocardial Infarction With Cardiogenic Shock in the United States
Abstract
Background: There are few studies evaluating regional disparities in the care of acute myocardial infarction-cardiogenic shock (AMI-CS).
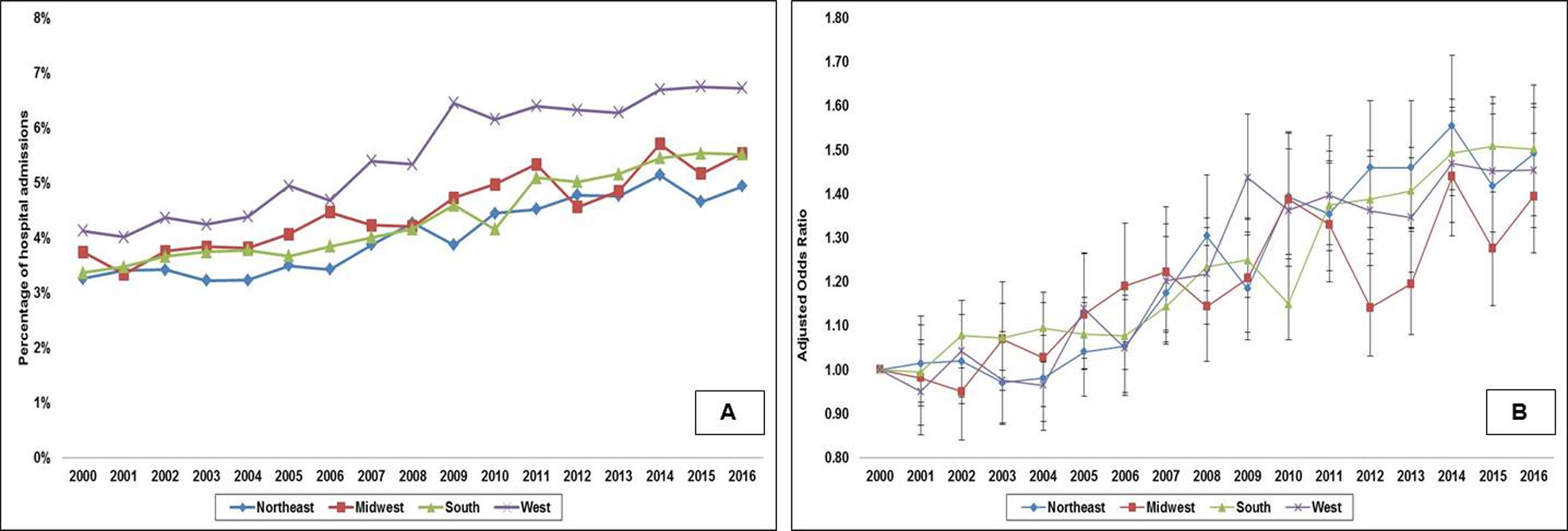
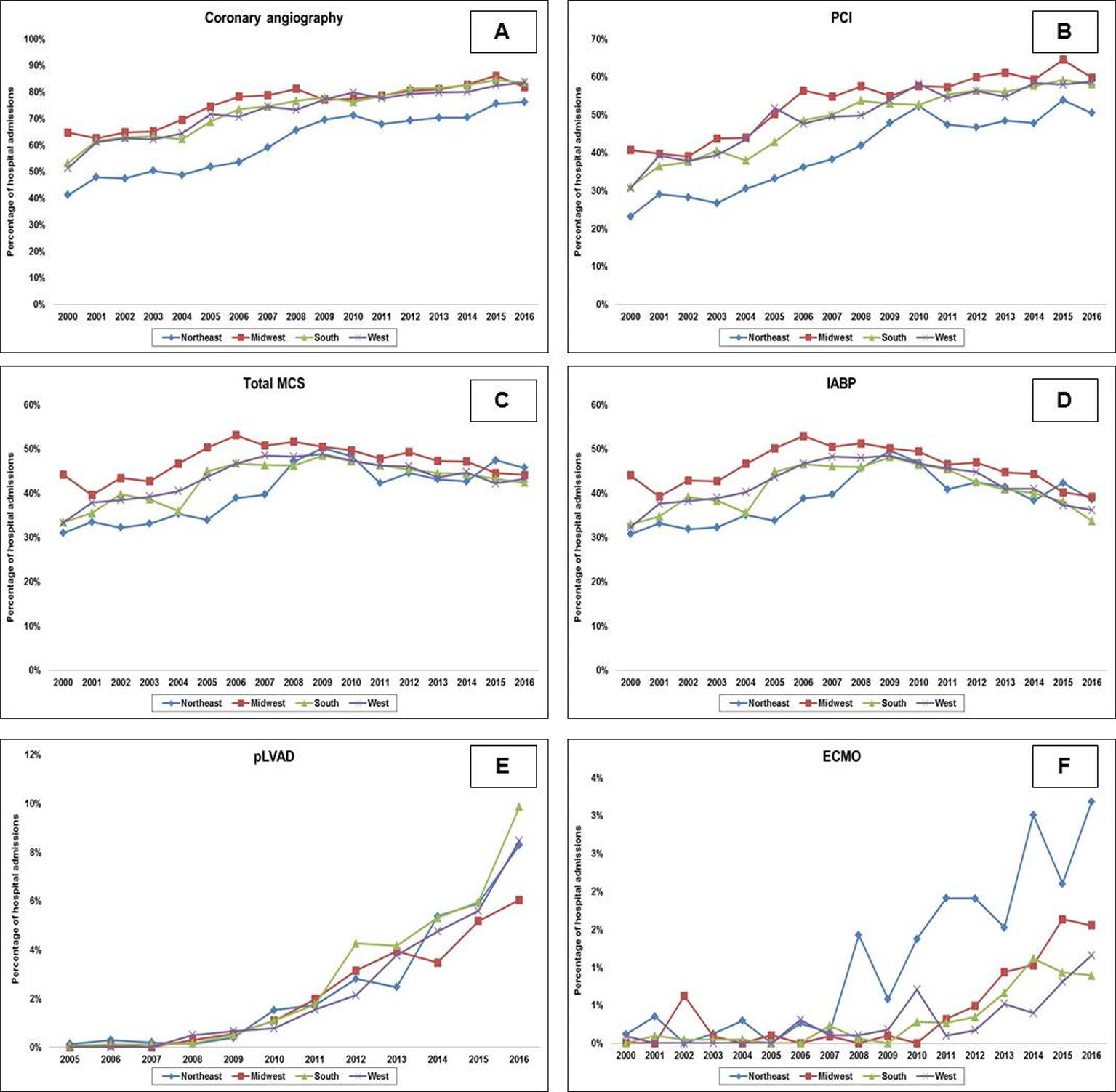
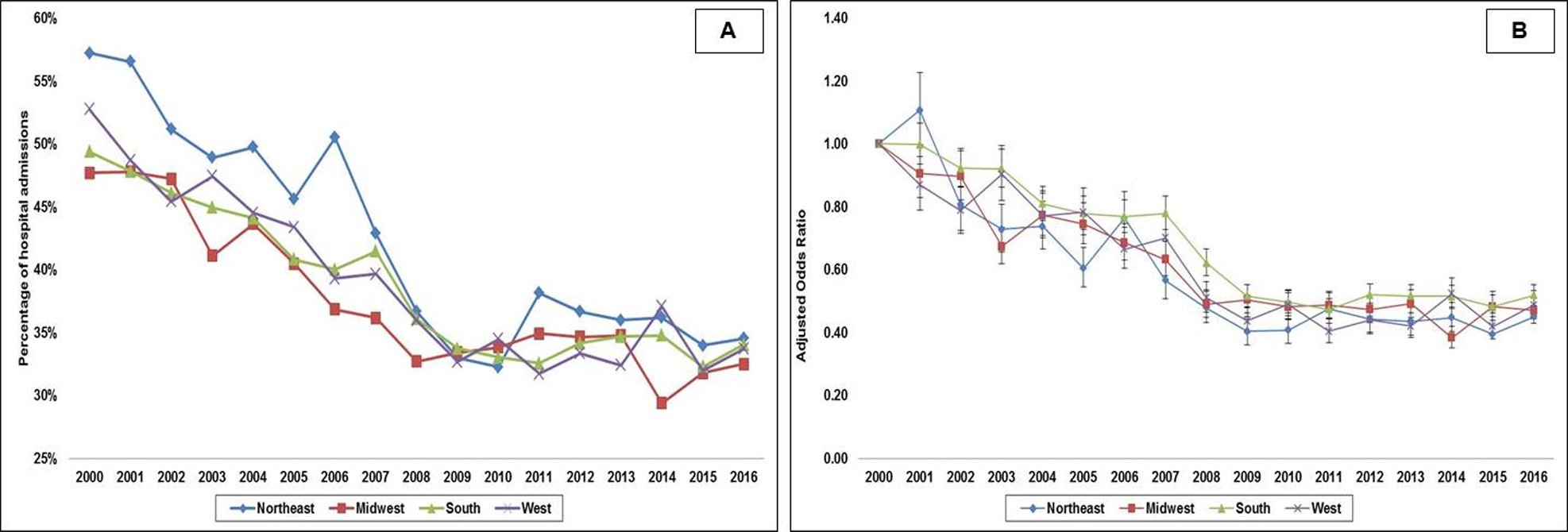
Methods and results: Using the National Inpatient Sample from 2000 to 2016, we identified adults with a primary diagnosis of AMI and concomitant CS admitted to the United States census regions of Northeast, Midwest, South, and West. Interhospital transfers were excluded. End points of interest included in-hospital mortality, use of coronary angiography, percutaneous coronary intervention, mechanical circulatory support, hospitalization costs, length of stay, and discharge disposition. Multivariable regression was used to adjust for potential confounding. Of the 402 825 AMI-CS admissions, 16.8%, 22.5%, 39.3%, and 21.4% were admitted to the Northeast, Midwest, South, and West, respectively. Higher rates of ST-elevation AMI-CS were noted in the Midwest and West. Admissions to the Northeast were on average characterized by a higher frequency of whites, Medicare beneficiaries, and lower rates of cardiac arrest. Admissions to the Northeast were less likely to receive coronary angiography, percutaneous coronary intervention, and mechanical circulatory support, despite the highest rates of extracorporeal membrane oxygenation use. Compared with the Northeast, in-hospital mortality was lower in the Midwest (adjusted odds ratio [aOR], 0.96 [95% CI, 0.93-0.98]; P<0.001) and West (aOR, 0.96 [95% CI, 0.94-0.98]; P=0.001) but higher in the South (aOR, 1.04 [95% CI, 1.01-1.06]; P=0.002). The Midwest (aOR, 1.68 [95% CI, 1.62-1.74]; P<0.001), South (aOR, 1.86 [95% CI, 1.80-1.92]; P<0.001), and West (aOR, 1.93 [95% CI, 1.86-2.00]; P<0.001) had higher discharges to home.
Conclusions: There remain significant regional disparities in the management and outcomes of AMI-CS.
Keywords: coronary angiography; hospitalization; length of stay; myocardial infarction; percutaneous coronary intervention.
Figures
References
-
- Vallabhajosyula S, Arora S, Lahewala S, Kumar V, Shantha GPS, Jentzer JC, Stulak JM, Gersh BJ, Gulati R, Rihal CS, Prasad A and Deshmukh AJ. Temporary mechanical circulatory support for refractory cardiogenic shock before left ventricular assist device surgery. J Am Heart Assoc. 2018;7:e010193. - PMC - PubMed
-
- Vallabhajosyula S, Arora S, Sakhuja A, Lahewala S, Kumar V, Shantha GPS, Egbe AC, Stulak JM, Gersh BJ, Gulati R, Rihal CS, Prasad A and Deshmukh AJ. Trends, predictors, and outcomes of temporary mechanical circulatory support for postcardiac surgery cardiogenic shock. Am J Cardiol. 2019;123:489–497. - PubMed
-
- Vallabhajosyula S, Dunlay SM, Barsness GW, Rihal CS, Holmes DR Jr. and Prasad A. Hospital-level disparities in the outcomes of acute myocardial infarction with cardiogenic shock. Am J Cardiol. 2019;124:491–498. - PubMed
-
- Vallabhajosyula S, Dunlay SM, Barsness GW, Vallabhajosyula S, Vallabhajosyula S, Sundaragiri PR, Gersh BJ, Jaffe AS and Kashani K. Temporal trends, predictors, and outcomes of acute kidney injury and hemodialysis use in acute myocardial infarction-related cardiogenic shock. PLoS One. 2019;14:e0222894. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
