

Optical coherence tomography features of retinal lesions in Chinese patients with endogenous Candida endophthalmitis
- PMID: 32059661
- PMCID: PMC7020574
- DOI: 10.1186/s12886-020-01337-9
Optical coherence tomography features of retinal lesions in Chinese patients with endogenous Candida endophthalmitis
Abstract
Background: To evaluate the optical coherence tomography (OCT) features of retinal lesions in Chinese patients with endogenous Candida endophthalmitis (ECE).
Methods: We performed a retrospective review of patients diagnosed with ECE at one medical center. The medical records of the patients including predisposing risk factors, treatment and visual acuity were reviewed. And we focused on the analysis of OCT images of retinal lesions before and after treatment.
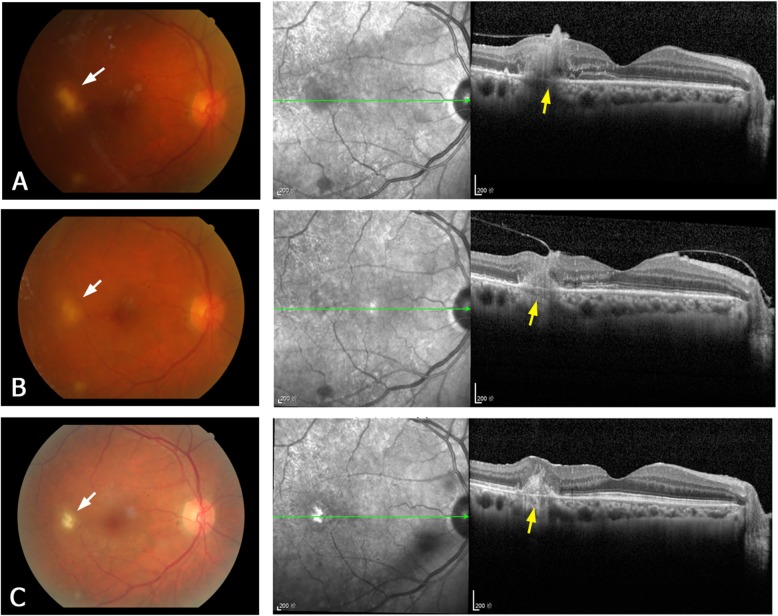
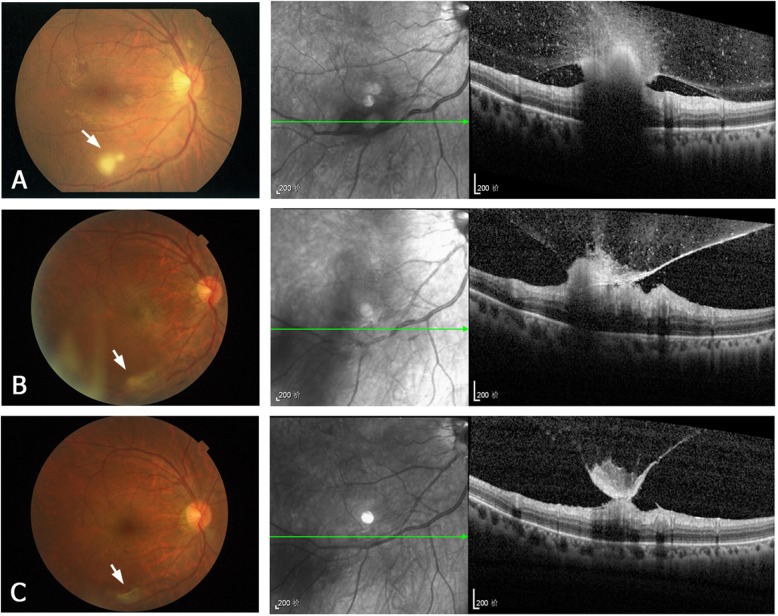
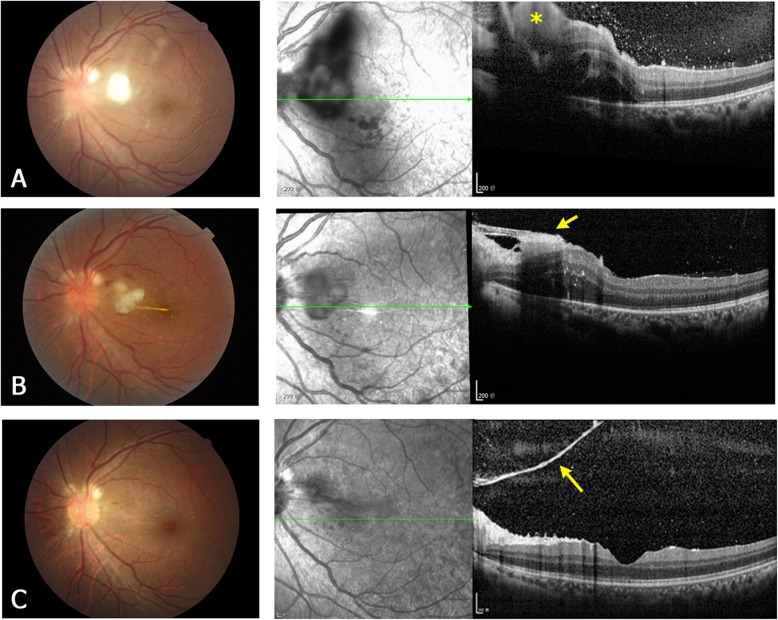
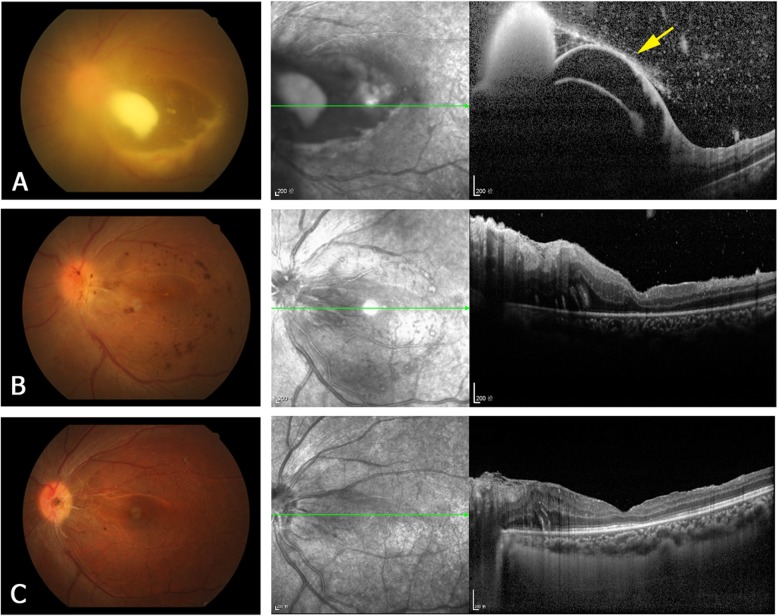
Results: A total of 16 Chinese patients (22 eyes) were included in this study. The most frequent predisposing risk factors were intravenous use of corticosteroids or antibiotics, lithotripsy for urinary calculi, and diabetes. After treatment, visual acuity was improved in 13 (59.1%) of the 22 eyes, and remained the same in the other 9 (40.9%) eyes. Pre-treatment OCT images obtained at presentation were available for 17 of the 22 eyes. Four types of the OCT manifestations of retinal lesions were identified: type 1 (subretinal macular lesions), type 2 (lesions are located in the inner retinal layer), type 3 (lesions involve the full-thickness retina and accompanied with macular edema), type 4 (sub-inner limiting membrane lesions). Pre-treatment OCT imaging of the 17 eyes revealed five as type 1, four as type 2, six as type 3, and two as type 4. After treatment, OCT images revealed epiretinal membrane and subretinal fibrosis as the most common post-treatment complications of ECE. Epiretinal membrane was detected in 2/4 type 2 lesions, in 4/6 type 3 lesions, and in 1/2 type 4 lesions, while subretinal fibrosis was mainly seen in type 1 lesions (4/5). Among the types, visual prognosis was best in eyes with type 2 lesions.
Conclusions: In this case series, the OCT manifestations of retinal lesions in ECE could be classified into four types. The post-treatment OCT manifestations were different in four types of lesions. We preliminarily found that the OCT morphology of retinal lesions was associated with the visual prognosis of ECE.
Keywords: Candida albicans; Endogenous endophthalmitis; Optical coherence tomography; Retinal lesion.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
