

Eosinophils, basophils and type 2 immune microenvironments in COPD-affected lung tissue
- PMID: 32060064
- PMCID: PMC7236868
- DOI: 10.1183/13993003.00110-2019
Eosinophils, basophils and type 2 immune microenvironments in COPD-affected lung tissue
Abstract
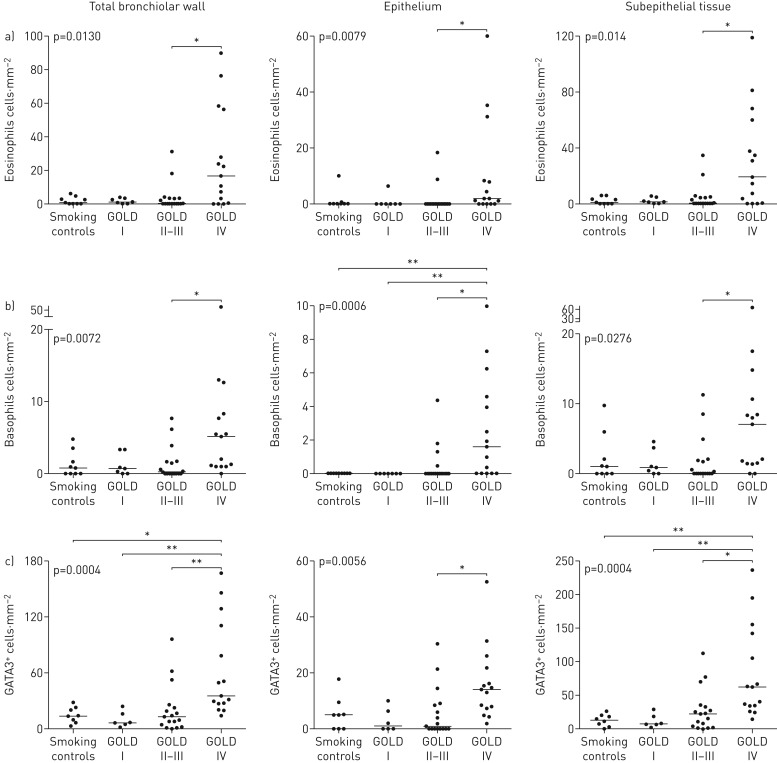
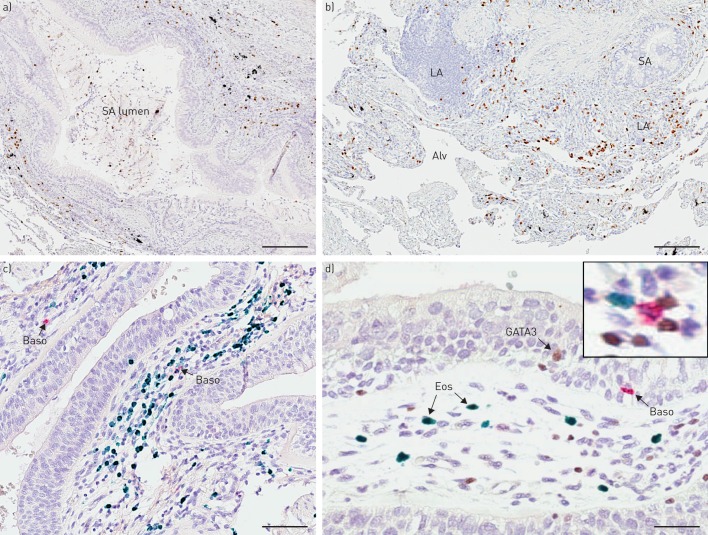
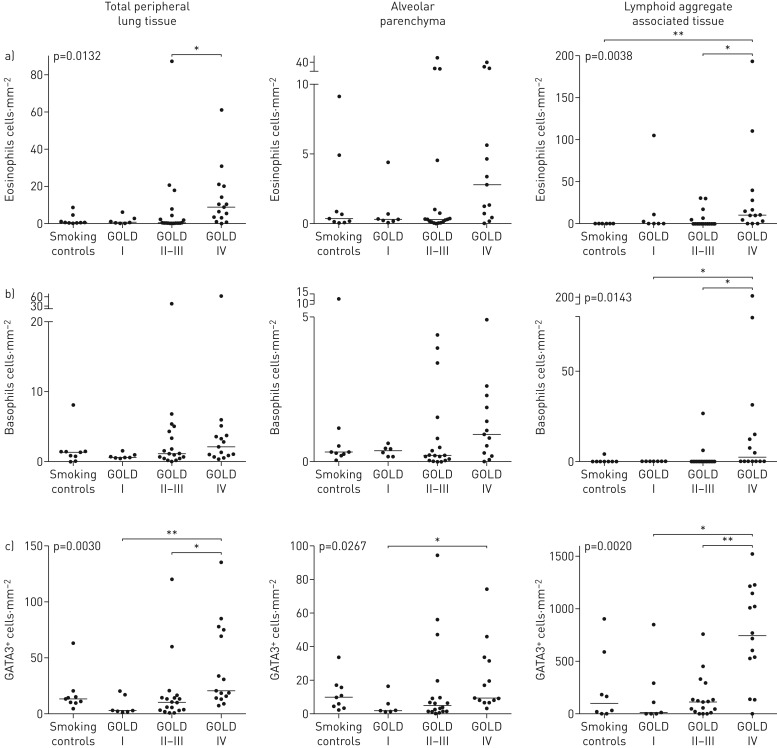
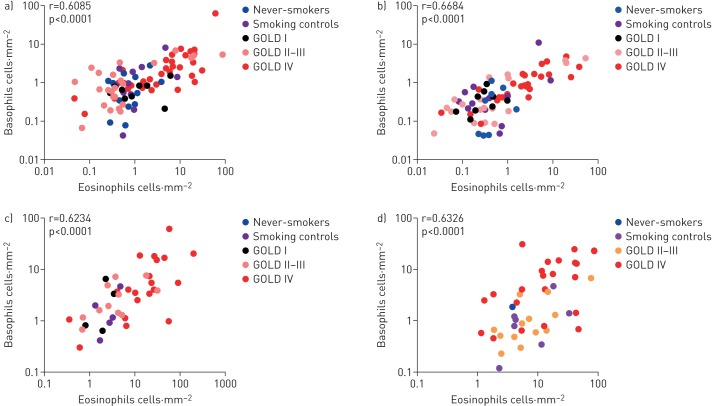
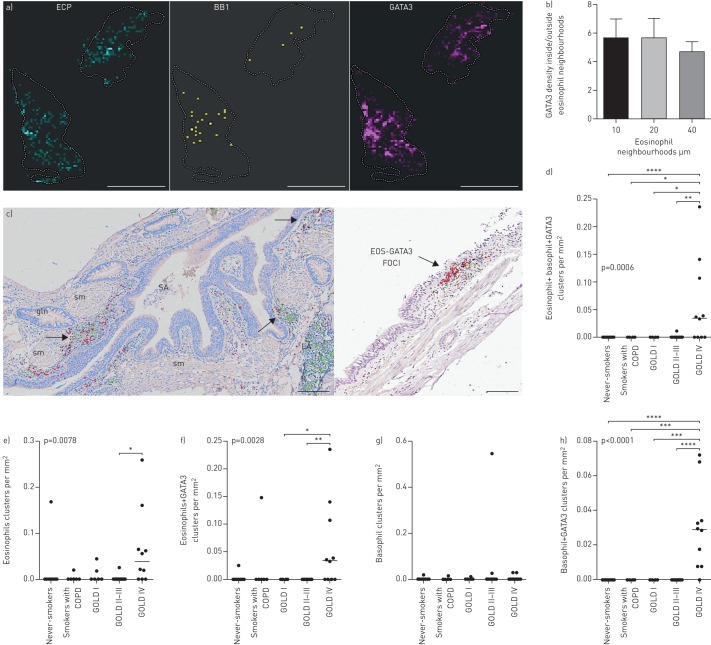
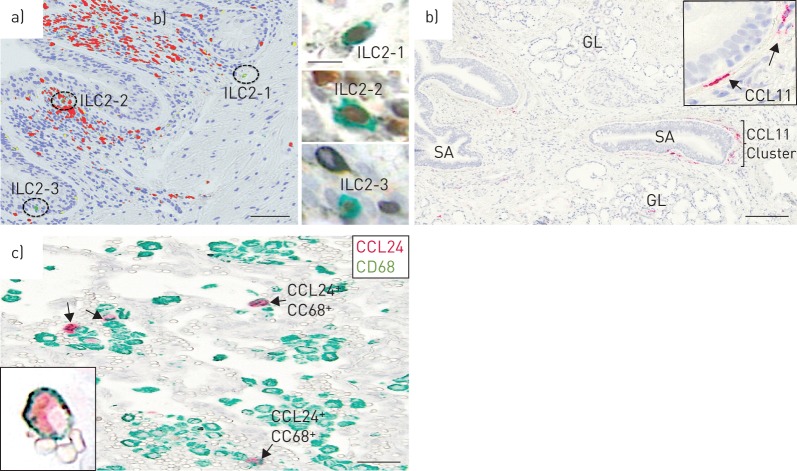
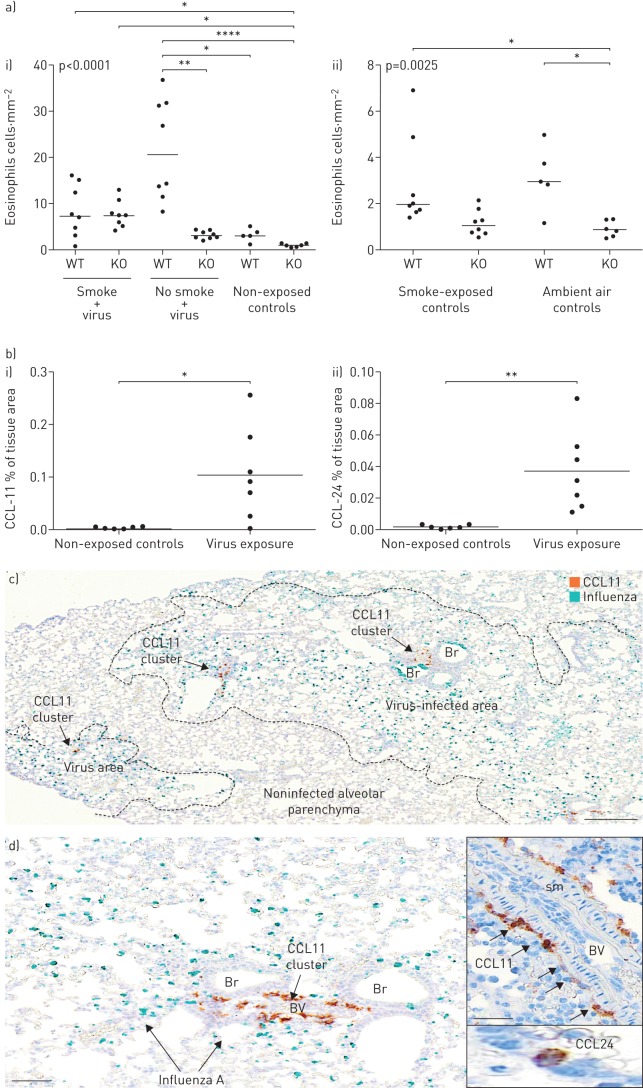
Although elevated blood or sputum eosinophils are present in many patients with COPD, uncertainties remain regarding the anatomical distribution pattern of lung-infiltrating eosinophils. Basophils have remained virtually unexplored in COPD. This study mapped tissue-infiltrating eosinophils, basophils and eosinophil-promoting immune mechanisms in COPD-affected lungs.Surgical lung tissue and biopsies from major anatomical compartments were obtained from COPD patients with severity grades Global Initiative for Chronic Obstructive Lung Disease stages I-IV; never-smokers/smokers served as controls. Automated immunohistochemistry and in situ hybridisation identified immune cells, the type 2 immunity marker GATA3 and eotaxins (CCL11, CCL24).Eosinophils and basophils were present in all anatomical compartments of COPD-affected lungs and increased significantly in very severe COPD. The eosinophilia was strikingly patchy, and focal eosinophil-rich microenvironments were spatially linked with GATA3+ cells, including type 2 helper T-cell lymphocytes and type 2 innate lymphoid cells. A similarly localised and interleukin-33/ST2-dependent eosinophilia was demonstrated in influenza-infected mice. Both mice and patients displayed spatially confined eotaxin signatures with CCL11+ fibroblasts and CCL24+ macrophages.In addition to identifying tissue basophilia as a novel feature of advanced COPD, the identification of spatially confined eosinophil-rich type 2 microenvironments represents a novel type of heterogeneity in the immunopathology of COPD that is likely to have implications for personalised treatment.
Copyright ©ERS 2020.
Conflict of interest statement
Conflict of interest: P. Jogdand has nothing to disclose. Conflict of interest: P. Siddhuraj has nothing to disclose. Conflict of interest: M. Mori has nothing to disclose. Conflict of interest: C. Sanden has nothing to disclose. Conflict of interest: J. Jönsson has nothing to disclose. Conflict of interest: A.F. Walls has nothing to disclose. Conflict of interest: J. Kearley is an employee of AstraZeneca (formerly MedImmune LLC) and has stock options in AstraZeneca. Conflict of interest: A.A. Humbles was an employee of AstraZeneca (formerly MedImmune LLC) at the time these analyses were conducted. Conflict of interest: R. Kolbeck was an employee of AstraZeneca (formerly MedImmune LLC) at the time these analyses were conducted. Conflict of interest: L. Bjermer has nothing to disclose. Conflict of interest: P. Newbold is an employee of AstraZeneca (formerly MedImmune LLC) and has stock options in AstraZeneca. Conflict of interest: J.S. Erjefält is founder (and stock owner) of Medetect AB, who received funding from AstraZeneca for conducting parts of the present study.
Figures
References
-
- Mori M, Andersson CK, Svedberg KA, et al. . Appearance of remodelled and dendritic cell-rich alveolar-lymphoid interfaces provides a structural basis for increased alveolar antigen uptake in chronic obstructive pulmonary disease. Thorax 2013; 68: 521–531. doi:10.1136/thoraxjnl-2012-202879 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical