

Disparities in glioblastoma survival by case volume: a nationwide observational study
- PMID: 32060840
- PMCID: PMC7136186
- DOI: 10.1007/s11060-020-03428-5
Disparities in glioblastoma survival by case volume: a nationwide observational study
Abstract
Introduction: High hospital case volumes are associated with improved treatment outcomes for numerous diseases. We assessed the association between academic non-profit hospital case volume and survival of adult glioblastoma patients.
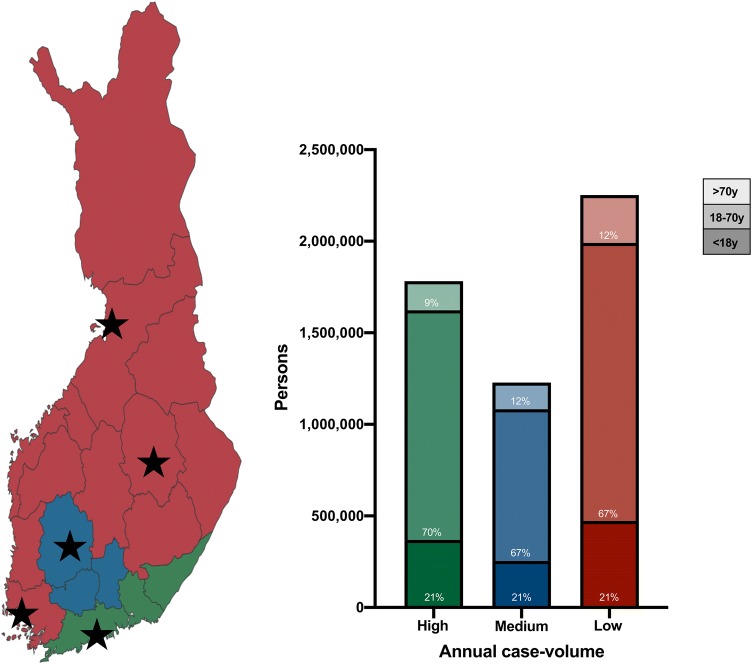
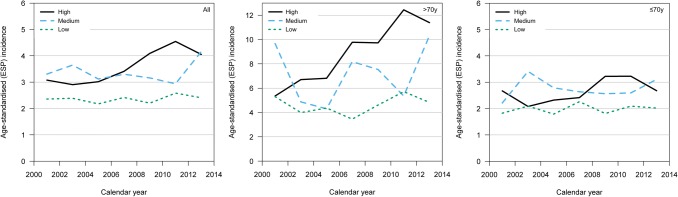
Methods: From the nationwide Finnish Cancer Registry, we identified all adult (≥ 18 years) patients with histopathological diagnoses of glioblastoma from 2000 to 2013. Five university hospitals (treating all glioblastoma patients in Finland) were classified as high-volume (one hospital), middle-volume (one hospital), and low-volume (three hospitals) based on their annual numbers of cases. We estimated one-year survival rates, estimated median overall survival times, and compared relative excess risk (RER) of death between high, middle, and low-volume hospitals.
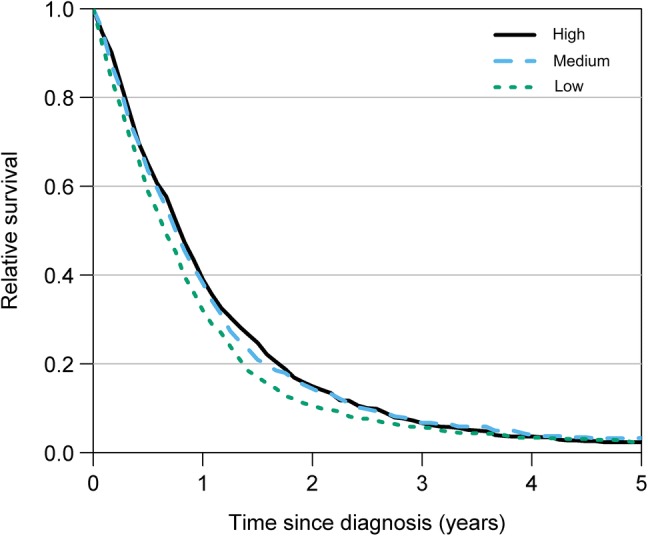
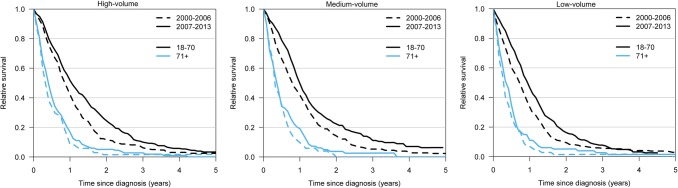
Results: A total of 2,045 patients were included. The mean numbers of annually treated patients were 54, 40, and 17 in the high, middle, and low-volume hospitals, respectively. One-year survival rates and median survival times were higher and longer in the high-volume (39%, 9.3 months) and medium-volume (38%, 8.9 months) hospitals than in the low-volume (32%, 7.8 months) hospitals. RER of death was higher in the low-volume hospitals than in the high-volume hospital (RER = 1.19, 95% CI 1.07-1.32, p = 0.002). There was no difference in RER of death between the high-volume and medium-volume hospitals (p = 0.690).
Conclusion: Higher glioblastoma case volumes were associated with improved survival. Future studies should assess whether this association is due to differences in patient-specific factors or treatment quality.
Keywords: Epidemiological study; Glioblastoma; Glioma; Malignant glioma; Mortality; Outcome.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
