

ACVIM consensus statement guidelines for the diagnosis, classification, treatment, and monitoring of pulmonary hypertension in dogs
- PMID: 32065428
- PMCID: PMC7097566
- DOI: 10.1111/jvim.15725
ACVIM consensus statement guidelines for the diagnosis, classification, treatment, and monitoring of pulmonary hypertension in dogs
Abstract
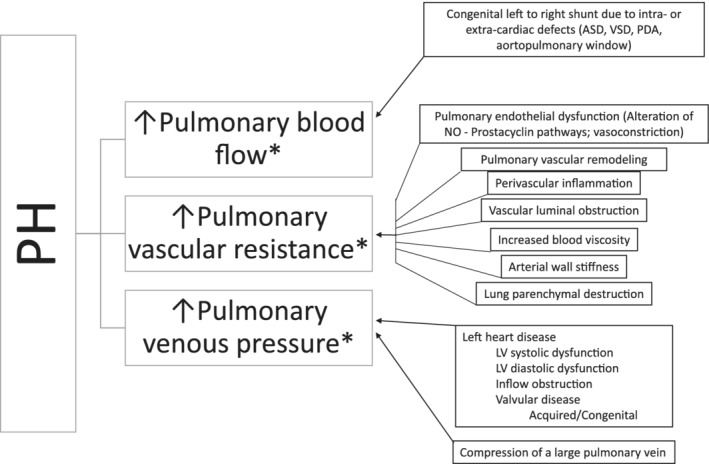
Pulmonary hypertension (PH), defined by increased pressure within the pulmonary vasculature, is a hemodynamic and pathophysiologic state present in a wide variety of cardiovascular, respiratory, and systemic diseases. The purpose of this consensus statement is to provide a multidisciplinary approach to guidelines for the diagnosis, classification, treatment, and monitoring of PH in dogs. Comprehensive evaluation including consideration of signalment, clinical signs, echocardiographic parameters, and results of other diagnostic tests supports the diagnosis of PH and allows identification of associated underlying conditions. Dogs with PH can be classified into the following 6 groups: group 1, pulmonary arterial hypertension; group 2, left heart disease; group 3, respiratory disease/hypoxia; group 4, pulmonary emboli/pulmonary thrombi/pulmonary thromboemboli; group 5, parasitic disease (Dirofilaria and Angiostrongylus); and group 6, disorders that are multifactorial or with unclear mechanisms. The approach to treatment of PH focuses on strategies to decrease the risk of progression, complications, or both, recommendations to target underlying diseases or factors contributing to PH, and PH-specific treatments. Dogs with PH should be monitored for improvement, static condition, or progression, and any identified underlying disorder should be addressed and monitored simultaneously.
Keywords: echocardiography; pulmonary arterial hypertension; respiratory disease; tricuspid regurgitation velocity.
© 2020 The Authors. Journal of Veterinary Internal Medicine published by Wiley Periodicals, Inc. on behalf of the American College of Veterinary Internal Medicine.
Conflict of interest statement
Carol Reinero received donation of medication (tadalafil) for an intramurally funded clinical trial comparing efficacy of sildenafil and tadalafil in dogs with pulmonary hypertension (2017‐2018). Brian Scansen has received speaking fees and travel expense reimbursement from Boehringer Ingelheim Animal Health. All other authors have no declared conflicts of interest.
Figures



References
-
- Thangaratinam S, Redman CWE. The Delphi technique. Obstet Gynaecol. 2005;7:120‐125.
-
- Hsu CC, Sandford BA. The Delphi technique: making sense of consensus. Pract Assess Res Eval. 2007;12:1‐7.
-
- Hoeper MM, Bogaard HJ, Condliffe R, et al. Definitions and diagnosis of pulmonary hypertension. J Am Coll Cardiol. 2013;62:D42‐D50. - PubMed
-
- Vachiery JL, Adir Y, Barbera JA, et al. Pulmonary hypertension due to left heart diseases. J Am Coll Cardiol. 2013;62:D100‐D108. - PubMed