

Effect of No Prehydration vs Sodium Bicarbonate Prehydration Prior to Contrast-Enhanced Computed Tomography in the Prevention of Postcontrast Acute Kidney Injury in Adults With Chronic Kidney Disease: The Kompas Randomized Clinical Trial
- PMID: 32065601
- PMCID: PMC7042862
- DOI: 10.1001/jamainternmed.2019.7428
Effect of No Prehydration vs Sodium Bicarbonate Prehydration Prior to Contrast-Enhanced Computed Tomography in the Prevention of Postcontrast Acute Kidney Injury in Adults With Chronic Kidney Disease: The Kompas Randomized Clinical Trial
Abstract
Importance: Prevention of postcontrast acute kidney injury in patients with stage 3 chronic kidney disease (CKD) by means of prehydration has been standard care for years. However, evidence for the need for prehydration in this group is limited.
Objective: To assess the renal safety of omitting prophylactic prehydration prior to iodine-based contrast media administration in patients with stage 3 CKD.
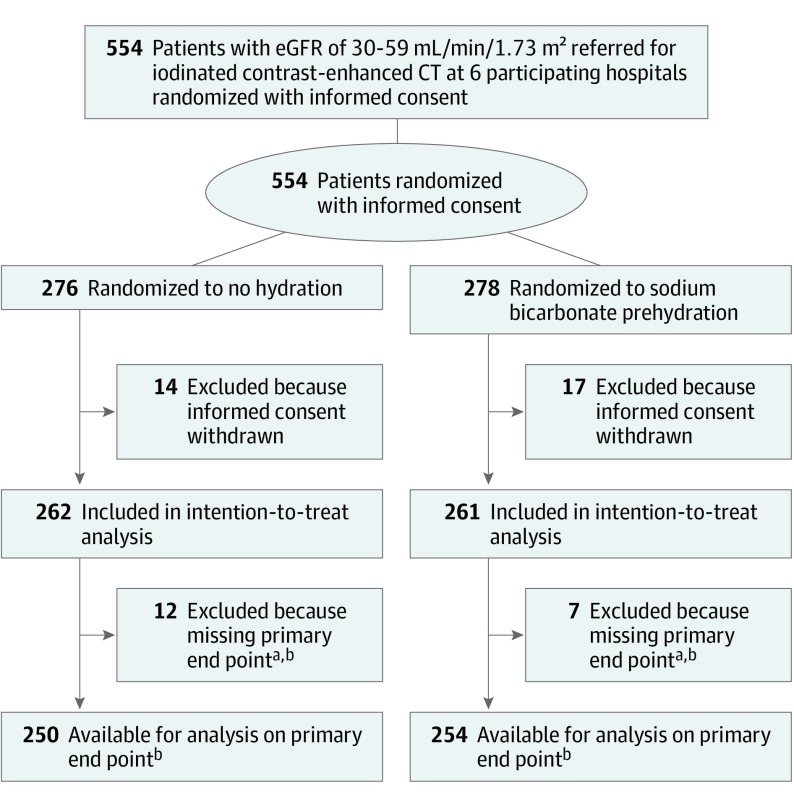
Design, setting, and participants: The Kompas trial was a multicenter, noninferiority, randomized clinical trial conducted at 6 hospitals in the Netherlands in which 523 patients with stage 3 CKD were randomized in a 1:1 ratio to receive no prehydration or prehydration with 250 mL of 1.4% sodium bicarbonate administered in a 1-hour infusion before undergoing elective contrast-enhanced computed tomography from April 2013 through September 2016. Final follow-up was completed in September 2017. Data were analyzed from January 2018 to June 2019.
Interventions: In total, 262 patients were allocated to the no prehydration group and 261 were allocated to receive prehydration. Analysis on the primary end point was available in 505 patients (96.6%).
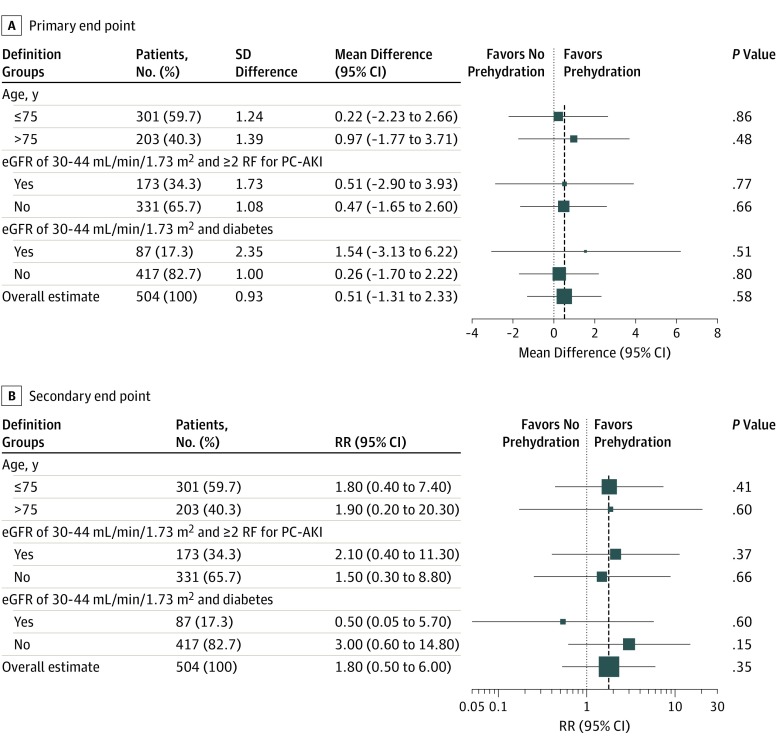
Main outcomes and measures: The primary end point was the mean relative increase in serum creatinine level 2 to 5 days after contrast administration compared with baseline (noninferiority margin of less than 10% increase in serum creatinine level). Secondary outcomes included the incidence of postcontrast acute kidney injury 2 to 5 days after contrast administration, mean relative increase in creatinine level 7 to 14 days after contrast administration, incidences of acute heart failure and renal failure requiring dialysis, and health care costs.
Results: Of 554 patients randomized, 523 were included in the intention-to-treat analysis. The median (interquartile range) age was 74 (67-79) years; 336 (64.2%) were men and 187 (35.8%) were women. The mean (SD) relative increase in creatinine level 2 to 5 days after contrast administration compared with baseline was 3.0% (10.5) in the no prehydration group vs 3.5% (10.3) in the prehydration group (mean difference, 0.5; 95% CI, -1.3 to 2.3; P < .001 for noninferiority). Postcontrast acute kidney injury occurred in 11 patients (2.1%), including 7 of 262 (2.7%) in the no prehydration group and 4 of 261 (1.5%) in the prehydration group, which resulted in a relative risk of 1.7 (95% CI, 0.5-5.9; P = .36). None of the patients required dialysis or developed acute heart failure. Subgroup analyses showed no evidence of statistical interactions between treatment arms and predefined subgroups. Mean hydration costs were €119 (US $143.94) per patient in the prehydration group compared with €0 (US $0) in the no prehydration group (P < .001). Other health care costs were similar.
Conclusions and relevance: Among patients with stage 3 CKD undergoing contrast-enhanced computed tomography, withholding prehydration did not compromise patient safety. The findings of this study support the option of not giving prehydration as a safe and cost-efficient measure.
Trial registration: Netherlands Trial Register Identifier: NTR3764.
Conflict of interest statement
Figures
Comment in
-
Nierenschwache Senioren müssen Kontrastmittel nicht fürchten : Hydrierung vor CT.MMW Fortschr Med. 2020 May;162(9):28. doi: 10.1007/s15006-020-0465-0. MMW Fortschr Med. 2020. PMID: 32405851 Review. German. No abstract available.
-
In patients with CKD having CT with contrast media, no prehydration and prehydration did not differ for AKI.Ann Intern Med. 2020 Jul 21;173(2):JC8. doi: 10.7326/ACPJ202007210-009. Ann Intern Med. 2020. PMID: 32687762
References
-
- van der Molen AJ, Reimer P, Dekkers IA, et al. Post-contrast acute kidney injury. part 2: risk stratification, role of hydration and other prophylactic measures, patients taking metformin and chronic dialysis patients: recommendations for updated ESUR Contrast Medium Safety Committee guidelines. Eur Radiol. 2018;28(7):2856-2869. doi: 10.1007/s00330-017-5247-4 - DOI - PMC - PubMed
-
- van der Molen AJ, Reimer P, Dekkers IA, et al. Post-contrast acute kidney injury—part 1: definition, clinical features, incidence, role of contrast medium and risk factors: recommendations for updated ESUR Contrast Medium Safety Committee guidelines. Eur Radiol. 2018;28(7):2845-2855. doi: 10.1007/s00330-017-5246-5 - DOI - PMC - PubMed
-
- ACR Committee on Drugs and Contrast Media ACR Manual on Contrast Media. 11th ed Version 10.3. Reston, VA: American College of Radiology; 2018.
