

Clinical risk factors and atherosclerotic plaque extent to define risk for major events in patients without obstructive coronary artery disease: the long-term coronary computed tomography angiography CONFIRM registry
- PMID: 32065624
- PMCID: PMC7821703
- DOI: 10.1093/ehjci/jez322
Clinical risk factors and atherosclerotic plaque extent to define risk for major events in patients without obstructive coronary artery disease: the long-term coronary computed tomography angiography CONFIRM registry
Abstract
Aims: In patients without obstructive coronary artery disease (CAD), we examined the prognostic value of risk factors and atherosclerotic extent.
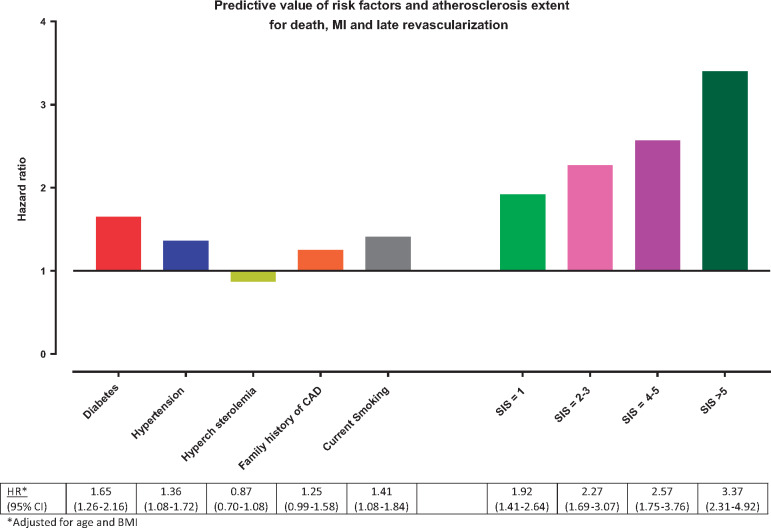
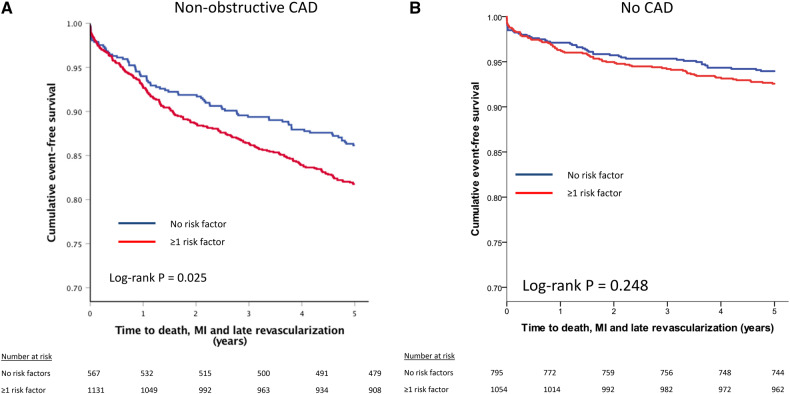
Methods and results: Patients from the long-term CONFIRM registry without prior CAD and without obstructive (≥50%) stenosis were included. Within the groups of normal coronary computed tomography angiography (CCTA) (N = 1849) and non-obstructive CAD (N = 1698), the prognostic value of traditional clinical risk factors and atherosclerotic extent (segment involvement score, SIS) was assessed with Cox models. Major adverse cardiac events (MACE) were defined as all-cause mortality, non-fatal myocardial infarction, or late revascularization. In total, 3547 patients were included (age 57.9 ± 12.1 years, 57.8% male), experiencing 460 MACE during 5.4 years of follow-up. Age, body mass index, hypertension, and diabetes were the clinical variables associated with increased MACE risk, but the magnitude of risk was higher for CCTA defined atherosclerotic extent; adjusted hazard ratio (HR) for SIS >5 was 3.4 (95% confidence interval [CI] 2.3-4.9) while HR for diabetes and hypertension were 1.7 (95% CI 1.3-2.2) and 1.4 (95% CI 1.1-1.7), respectively. Exclusion of revascularization as endpoint did not modify the results. In normal CCTA, presence of ≥1 traditional risk factors did not worsen prognosis (log-rank P = 0.248), while it did in non-obstructive CAD (log-rank P = 0.025). Adjusted for SIS, hypertension and diabetes predicted MACE risk in non-obstructive CAD, while diabetes did not increase risk in absence of CAD (P-interaction = 0.004).
Conclusion: Among patients without obstructive CAD, the extent of CAD provides more prognostic information for MACE than traditional cardiovascular risk factors. An interaction was observed between risk factors and CAD burden, suggesting synergistic effects of both.
Keywords: atherosclerosis; coronary computed tomography angiography; imaging; preventive cardiology; risk stratification.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author(s) 2020. For permissions, please email: journals.permissions@oup.com.
Figures
Comment in
-
Non-obstructive coronary artery disease can no longer be ignored.Eur Heart J Cardiovasc Imaging. 2020 May 1;21(5):489-490. doi: 10.1093/ehjci/jeaa022. Eur Heart J Cardiovasc Imaging. 2020. PMID: 32068781 No abstract available.
Similar articles
-
Long-term prognostic utility of computed tomography coronary angiography in older populations.Eur Heart J Cardiovasc Imaging. 2019 Nov 1;20(11):1279-1286. doi: 10.1093/ehjci/jez067. Eur Heart J Cardiovasc Imaging. 2019. PMID: 30993334
-
Predictive Value of Age- and Sex-Specific Nomograms of Global Plaque Burden on Coronary Computed Tomography Angiography for Major Cardiac Events.Circ Cardiovasc Imaging. 2017 Mar;10(3):e004896. doi: 10.1161/CIRCIMAGING.116.004896. Circ Cardiovasc Imaging. 2017. PMID: 28292858
-
Sex-Specific Associations Between Coronary Artery Plaque Extent and Risk of Major Adverse Cardiovascular Events: The CONFIRM Long-Term Registry.JACC Cardiovasc Imaging. 2016 Apr;9(4):364-372. doi: 10.1016/j.jcmg.2016.02.010. JACC Cardiovasc Imaging. 2016. PMID: 27056154 Free PMC article.
-
Prognostic value of segment involvement score compared to other measures of coronary atherosclerosis by computed tomography: A systematic review and meta-analysis.J Cardiovasc Comput Tomogr. 2017 Jul-Aug;11(4):258-267. doi: 10.1016/j.jcct.2017.05.001. Epub 2017 May 3. J Cardiovasc Comput Tomogr. 2017. PMID: 28483581
-
Utilizing (serial) coronary computed tomography angiography (CCTA) to predict plaque progression and major adverse cardiac events (MACE): results, merits and challenges.Eur Radiol. 2022 May;32(5):3408-3422. doi: 10.1007/s00330-021-08393-9. Epub 2022 Jan 8. Eur Radiol. 2022. PMID: 34997285 Review.
Cited by
-
Comparing predictive risk to actual presence of coronary atherosclerosis on coronary computed tomography angiography.Am Heart J Plus. 2024 Dec 6;49:100493. doi: 10.1016/j.ahjo.2024.100493. eCollection 2025 Jan. Am Heart J Plus. 2024. PMID: 39760104 Free PMC article.
-
Atherosclerosis quantification and cardiovascular risk: the ISCHEMIA trial.Eur Heart J. 2024 Sep 29;45(36):3735-3747. doi: 10.1093/eurheartj/ehae471. Eur Heart J. 2024. PMID: 39101625 Free PMC article. Clinical Trial.
-
The Quantification of Total Coronary Atheroma Burden - A Major Step Forward.Heart Int. 2020 Dec 23;14(2):73-75. doi: 10.17925/HI.2020.14.2.73. eCollection 2020. Heart Int. 2020. PMID: 36276513 Free PMC article. Review.
-
Prognostic value of coronary CT angiography for the prediction of all-cause mortality and non-fatal myocardial infarction: a propensity score analysis.Int J Cardiovasc Imaging. 2023 Nov;39(11):2247-2254. doi: 10.1007/s10554-023-02918-7. Epub 2023 Aug 17. Int J Cardiovasc Imaging. 2023. PMID: 37589870
-
Apolipoprotein B is associated with CT-angiographic progression beyond low-density lipoprotein cholesterol and non-high-density lipoprotein cholesterol in patients with coronary artery disease.Lipids Health Dis. 2023 Aug 9;22(1):125. doi: 10.1186/s12944-023-01872-6. Lipids Health Dis. 2023. PMID: 37559117 Free PMC article.
References
-
- Cury RC, Abbara S, Achenbach S, Agatston A, Berman DS, Budoff MJ et al. Coronary Artery Disease–Reporting and Data System (CAD-RADS): an Expert Consensus Document of SCCT, ACR and NASCI: endorsed by the ACC. JACC Cardiovasc Imaging 2016;9:1099–113. - PubMed
-
- Min JK, Dunning A, Lin FY, Achenbach S, Al-Mallah MH, Berman DS et al. Rationale and design of the CONFIRM (COronary CT Angiography EvaluatioN For Clinical Outcomes: an InteRnational Multicenter) registry. J Cardiovasc Comput Tomogr 2011;5:84–92. - PubMed
-
- Hoffmann U, Ferencik M, Udelson JE, Picard MH, Truong QA, Patel MR et al. Prognostic value of noninvasive cardiovascular testing in patients with stable chest pain: insights from the PROMISE Trial (Prospective Multicenter Imaging Study for Evaluation of Chest Pain). Circulation 2017;135:2320–32. - PMC - PubMed
-
- Min JK, Shaw LJ, Devereux RB, Okin PM, Weinsaft JW, Russo DJ et al. Prognostic value of multidetector coronary computed tomographic angiography for prediction of all-cause mortality. J Am Coll Cardiol 2007;50:1161–70. - PubMed
