

Adverse Effects of Low-Dose Methotrexate: A Randomized Trial
- PMID: 32066146
- PMCID: PMC7229518
- DOI: 10.7326/M19-3369
Adverse Effects of Low-Dose Methotrexate: A Randomized Trial
Abstract
Background: Low-dose methotrexate (LD-MTX) is the most commonly used drug for systemic rheumatic diseases worldwide and is the recommended first-line agent for rheumatoid arthritis. Despite extensive clinical use for more than 30 years, few data on adverse event (AE) rates derive from randomized, placebo-controlled trials, where both causality and magnitude of risk can be inferred.
Objective: To investigate AE rates, risk, and risk differences comparing LD-MTX versus placebo.
Design: Prespecified secondary analyses of a double-blind, placebo-controlled, randomized trial. (ClinicalTrials.gov: NCT01594333).
Setting: North America.
Participants: Adults with known cardiovascular disease and diabetes or metabolic syndrome.
Intervention: Random allocation to LD-MTX (≤20 mg/wk) or placebo. All participants received folic acid, 1 mg/d, 6 days per week.
Measurements: Risks for specific AEs of interest, as well as for all AEs, were compared across treatment groups after blinded adjudication.
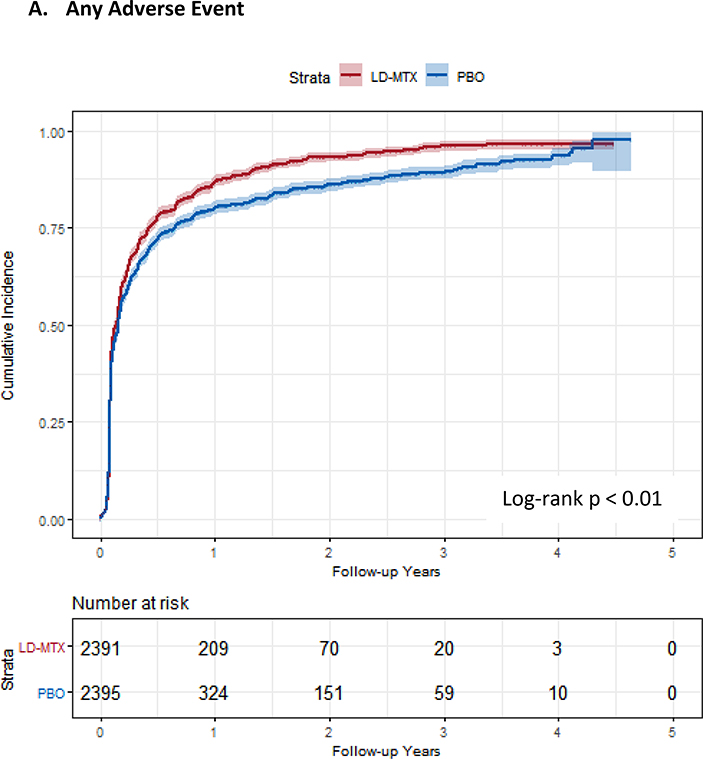
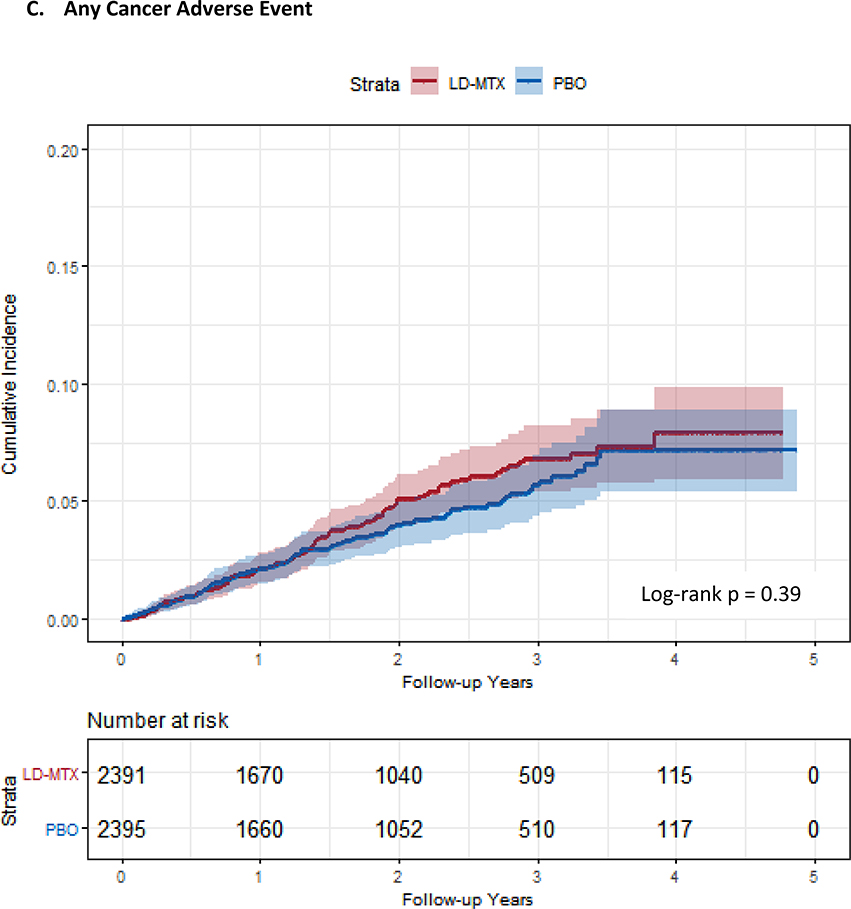
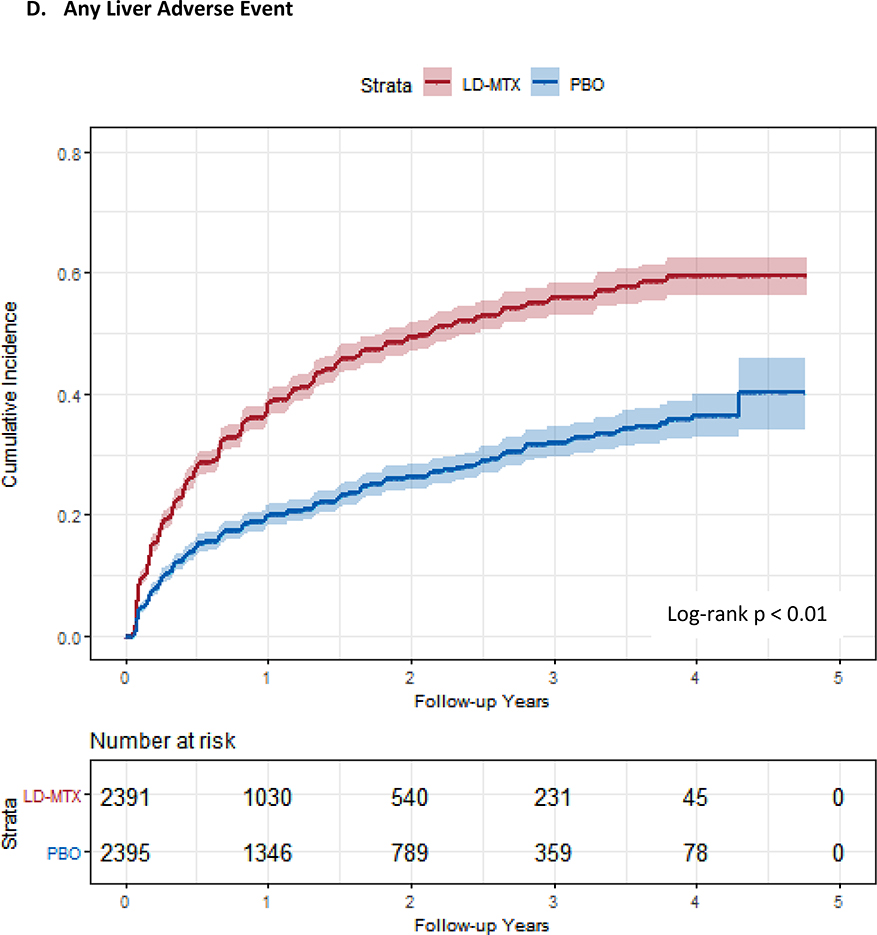
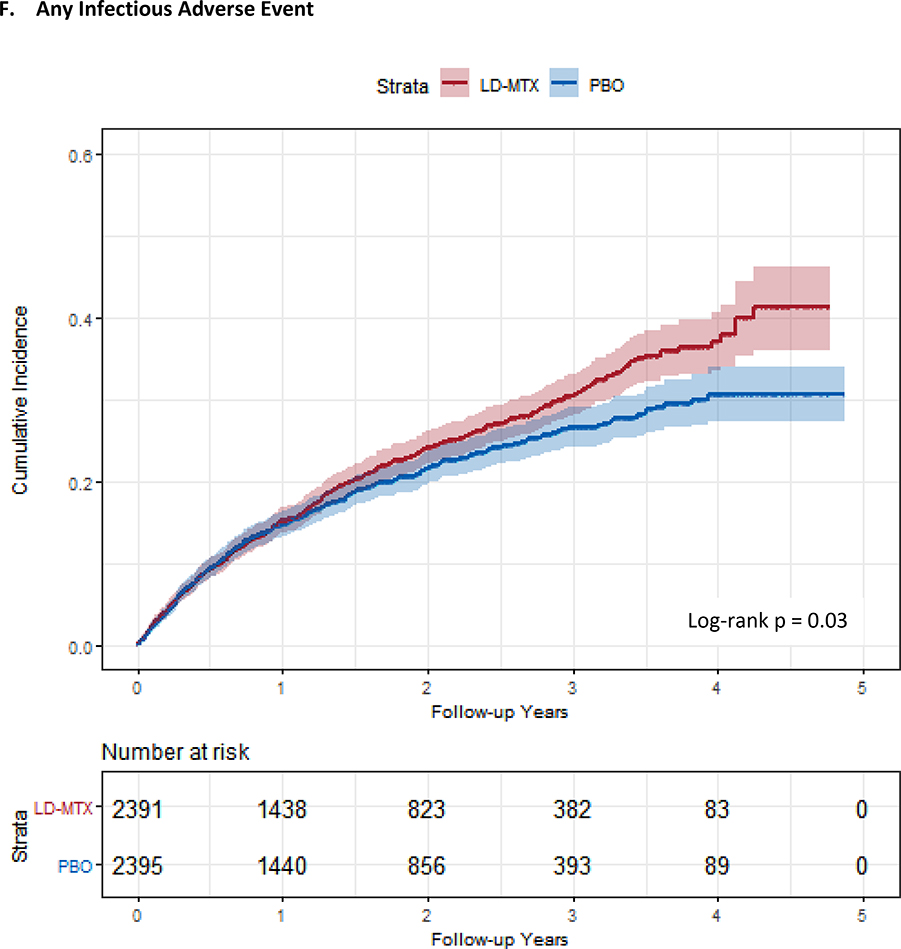
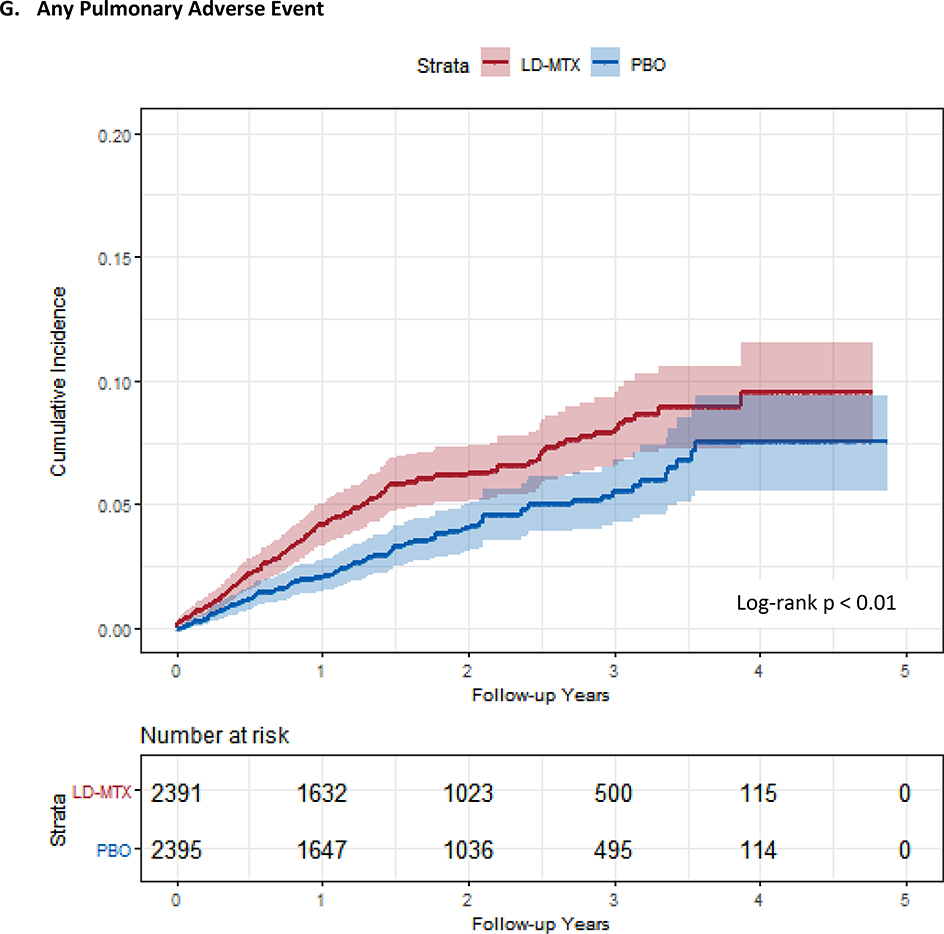
Results: After an active run-in period, 6158 patients were enrolled and 4786 randomly assigned to a group; median follow-up was 23 months and median dosage 15 mg/wk. Among the randomly assigned participants, 81.2% were male, median age was 65.7 years, and median body mass index was 31.5 kg/m2. Of 2391 participants assigned to LD-MTX, 2080 (87.0%) had an AE of interest, compared with 1951 of 2395 (81.5%) assigned to placebo (hazard ratio [HR], 1.17 [95% CI, 1.10 to 1.25]). The relative hazards of gastrointestinal (HR, 1.91 [CI, 1.75 to 2.10]), pulmonary (HR, 1.52 [CI, 1.16 to 1.98]), infectious (HR, 1.15 [CI, 1.01 to 1.30]), and hematologic (HR, 1.15 [CI, 1.07 to 1.23]) AEs were elevated for LD-MTX versus placebo. With the exception of increased risk for skin cancer (HR, 2.05 [CI, 1.28 to 3.28]), the treatment groups did not differ in risk for other cancer or mucocutaneous, neuropsychiatric, or musculoskeletal AEs. Renal AEs were reduced in the LD-MTX group (HR, 0.85 [CI, 0.78 to 0.93]).
Limitation: The trial was done in patients without rheumatic disease who tolerated LD-MTX during an active run-in period.
Conclusion: Use of LD-MTX was associated with small to moderate elevations in risks for skin cancer and gastrointestinal, infectious, pulmonary, and hematologic AEs, whereas renal AEs were decreased.
Primary funding source: National Institutes of Health.
Figures


Comment in
-
Adverse Effects of Low-Dose Methotrexate.Ann Intern Med. 2020 Jul 21;173(2):167. doi: 10.7326/L20-0525. Ann Intern Med. 2020. PMID: 32687751 No abstract available.
-
Adverse Effects of Low-Dose Methotrexate.Ann Intern Med. 2020 Jul 21;173(2):166-167. doi: 10.7326/L20-0524. Ann Intern Med. 2020. PMID: 32687752 No abstract available.
References
-
- Sparks JA, Barbhaiya M, Karlson EW, Ritter SY, Raychaudhuri S, Corrigan CC, et al. Investigating methotrexate toxicity within a randomized double-blinded, placebo-controlled trial: Rationale and design of the Cardiovascular Inflammation Reduction Trial-Adverse Events (CIRT-AE) Study. Semin Arthritis Rheum. 2017;47(1):133–42. - PMC - PubMed
-
- Finckh A, Liang MH, van Herckenrode CM, de Pablo P. Long-term impact of early treatment on radiographic progression in rheumatoid arthritis: A meta-analysis. Arthritis Rheum. 2006;55(6):864–72. - PubMed
-
- Weinblatt ME, Coblyn JS, Fox DA, Fraser PA, Holdsworth DE, Glass DN, et al. Efficacy of low-dose methotrexate in rheumatoid arthritis. N Engl J Med. 1985;312(13):818–22. - PubMed
-
- Weinblatt ME, Maier AL, Fraser PA, Coblyn JS. Longterm prospective study of methotrexate in rheumatoid arthritis: conclusion after 132 months of therapy. J Rheumatol. 1998;25(2):238–42. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials