

The pan-cancer landscape of prognostic germline variants in 10,582 patients
- PMID: 32066500
- PMCID: PMC7027124
- DOI: 10.1186/s13073-020-0718-7
The pan-cancer landscape of prognostic germline variants in 10,582 patients
Abstract
Background: While clinical factors such as age, grade, stage, and histological subtype provide physicians with information about patient prognosis, genomic data can further improve these predictions. Previous studies have shown that germline variants in known cancer driver genes are predictive of patient outcome, but no study has systematically analyzed multiple cancers in an unbiased way to identify genetic loci that can improve patient outcome predictions made using clinical factors.
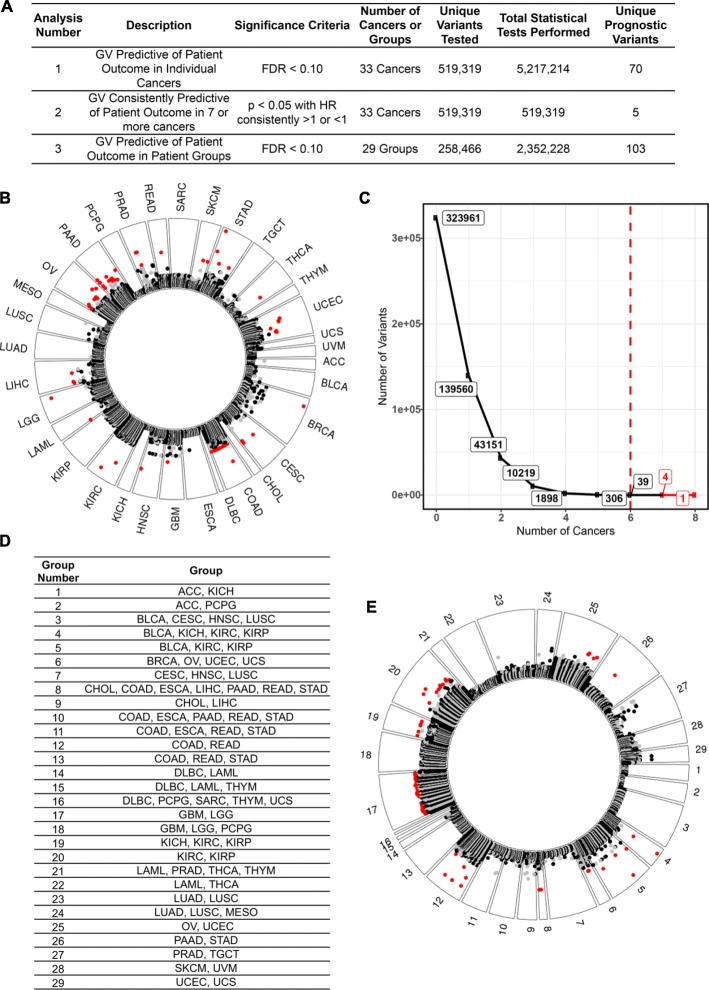
Methods: We analyzed sequencing data from the over 10,000 cancer patients available through The Cancer Genome Atlas to identify germline variants associated with patient outcome using multivariate Cox regression models.
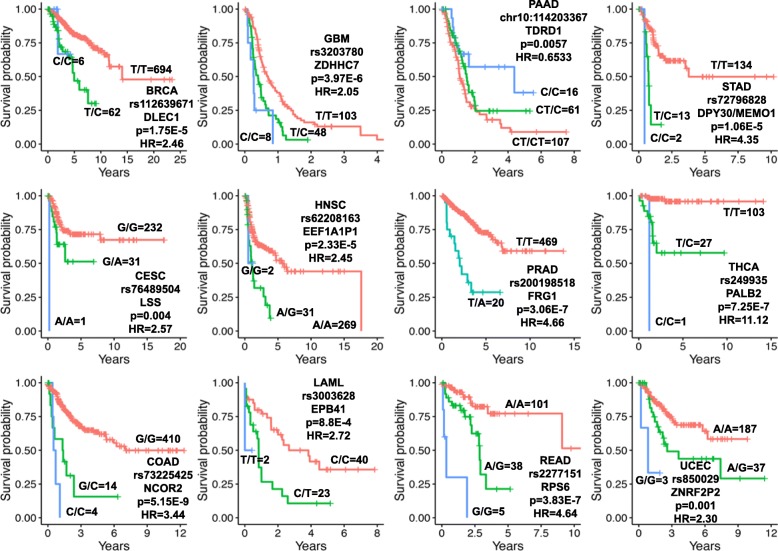
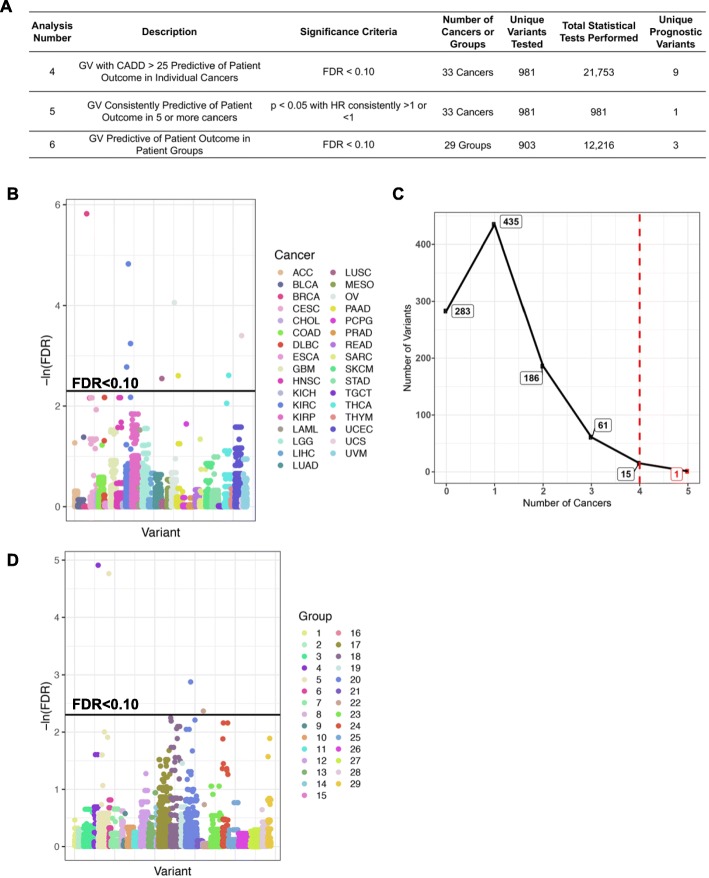
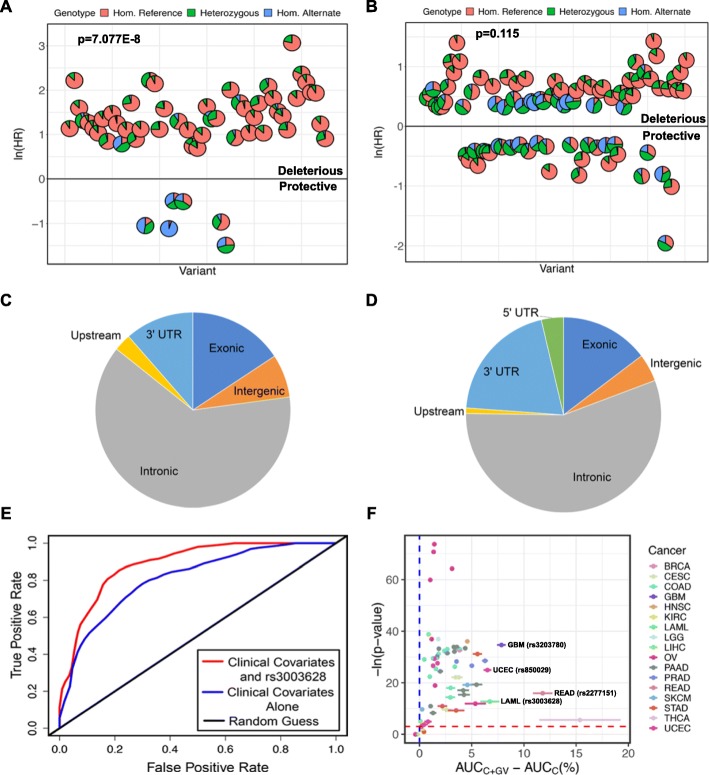
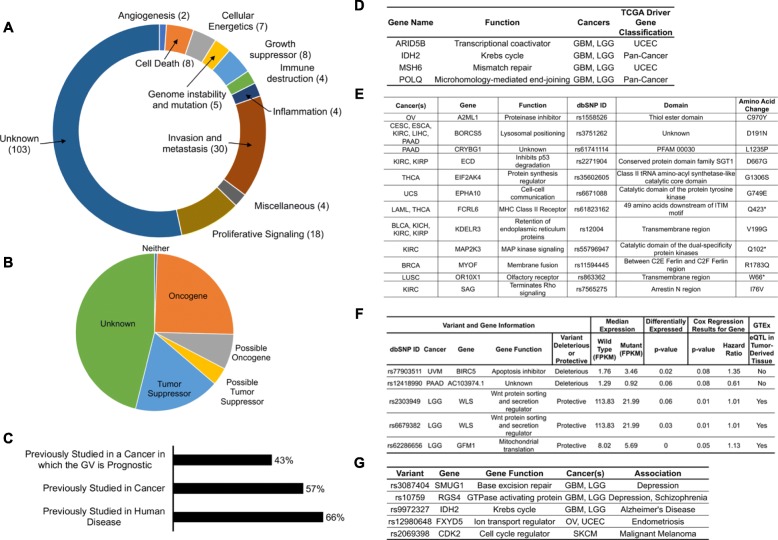
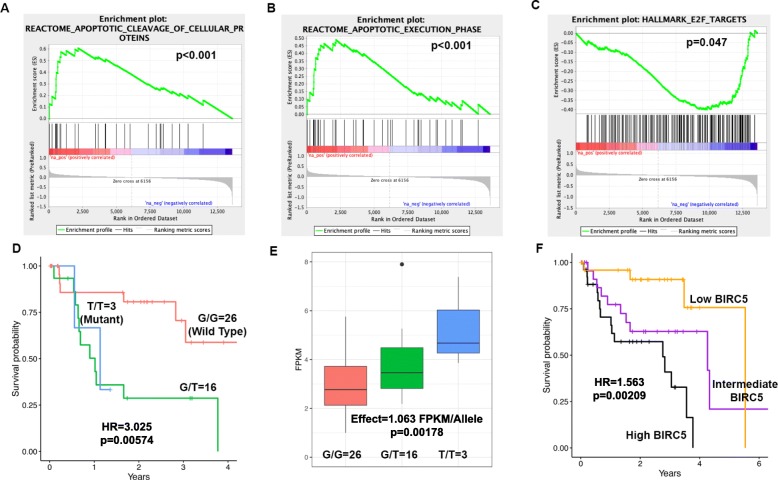
Results: We identified 79 prognostic germline variants in individual cancers and 112 prognostic germline variants in groups of cancers. The germline variants identified in individual cancers provide additional predictive power about patient outcomes beyond clinical information currently in use and may therefore augment clinical decisions based on expected tumor aggressiveness. Molecularly, at least 12 of the germline variants are likely associated with patient outcome through perturbation of protein structure and at least five through association with gene expression differences. Almost half of these germline variants are in previously reported tumor suppressors, oncogenes or cancer driver genes with the other half pointing to genomic loci that should be further investigated for their roles in cancers.
Conclusions: Germline variants are predictive of outcome in cancer patients and specific germline variants can improve patient outcome predictions beyond predictions made using clinical factors alone. The germline variants also implicate new means by which known oncogenes, tumor suppressor genes, and driver genes are perturbed in cancer and suggest roles in cancer for other genes that have not been extensively studied in oncology. Further studies in other cancer cohorts are necessary to confirm that germline variation is associated with outcome in cancer patients as this is a proof-of-principle study.
Keywords: Cancer biology; Driver gene; Germline variants; Non-synonymous mutation; Oncogene; Pan-cancer; Single nucleotide polymorphism; Survival analysis; Tumor suppressor; eQTL.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
