

Four-point impedance as a biomarker for bleeding during cochlear implantation
- PMID: 32066743
- PMCID: PMC7026160
- DOI: 10.1038/s41598-019-56253-w
Four-point impedance as a biomarker for bleeding during cochlear implantation
Abstract
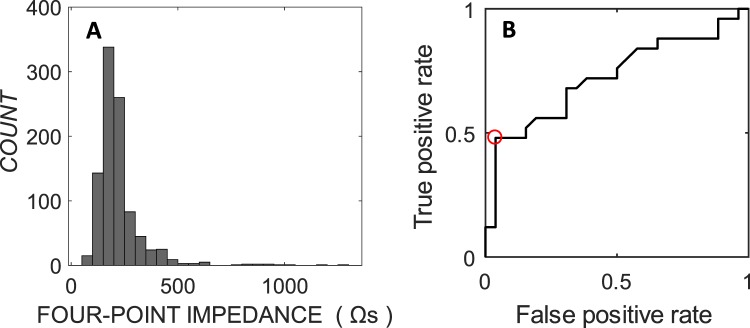
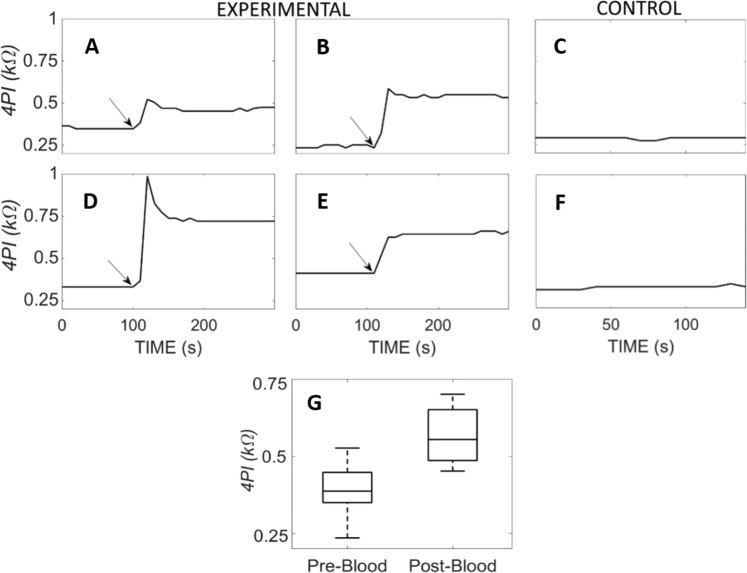
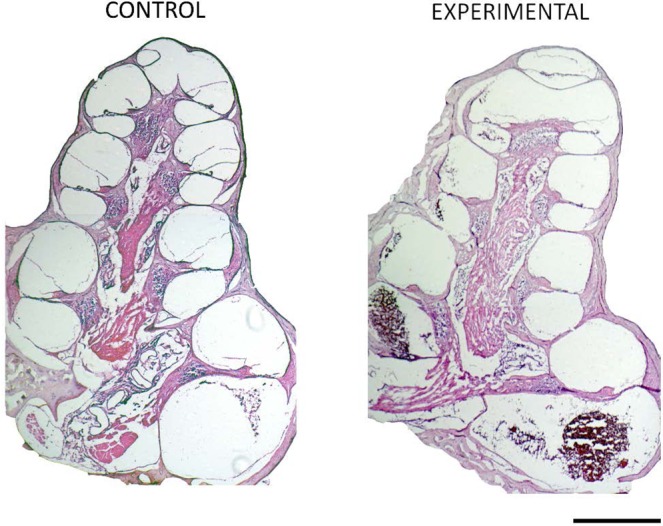
Cochlear implantation has successfully restored the perception of hearing for nearly 200 thousand profoundly deaf adults and children. More recently, implant candidature has expanded to include those with considerable natural hearing which, when preserved, provides an improved hearing experience in noisy environments. But more than half of these patients lose this natural hearing soon after implantation. To reduce this burden, biosensing technologies are emerging that provide feedback on the quality of surgery. Here we report clinical findings on a new intra-operative measurement of electrical impedance (4-point impedance) which, when elevated, is associated with high rates of post-operative hearing loss and vestibular dysfunction. In vivo and in vitro data presented suggest that elevated 4-point impedance is likely due to the presence of blood within the cochlea rather than its geometry. Four-point impedance is a new marker for the detection of cochlear injury causing bleeding, that may be incorporated into intraoperative monitoring protocols during CI surgery.
Conflict of interest statement
The authors declare no competing interests.
Figures



References
-
- Golub JS, et al. Spectral and temporal measures in hybrid cochlear implant users: on the mechanism of electroacoustic hearing benefits. Otology & neurotology: official publication of the American Otological Society, American Neurotology Society [and] European Academy of Otology and Neurotology. 2012;33(2):147. doi: 10.1097/MAO.0b013e318241b6d3. - DOI - PMC - PubMed
-
- Novartis. Hearing Restoration Clinical Trial. NCT02132130: (2014)
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
