

Characteristics of Atrial Fibrillation Patients Suffering Esophageal Injury Caused by Ablation for Atrial Fibrillation
- PMID: 32066780
- PMCID: PMC7026048
- DOI: 10.1038/s41598-020-59539-6
Characteristics of Atrial Fibrillation Patients Suffering Esophageal Injury Caused by Ablation for Atrial Fibrillation
Abstract
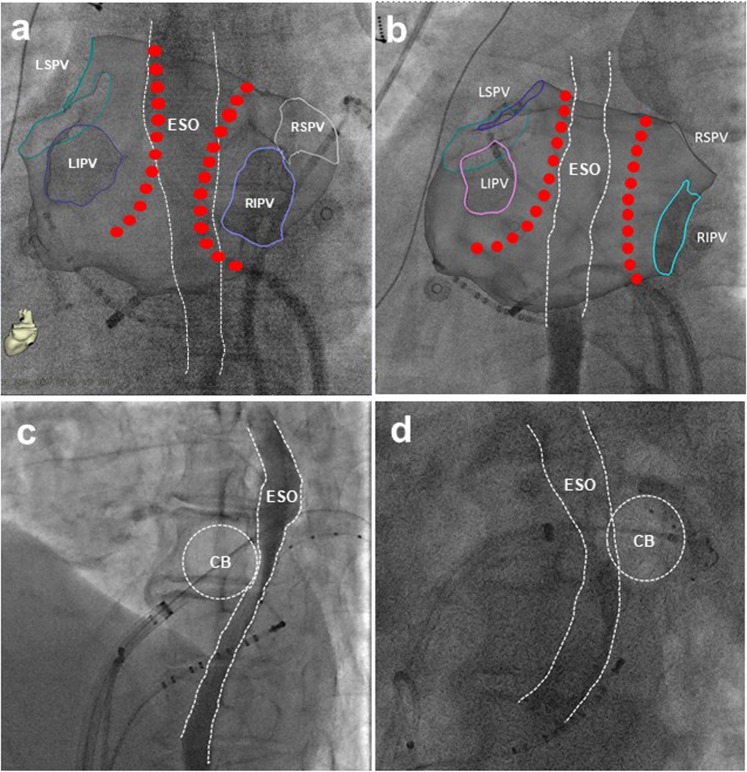
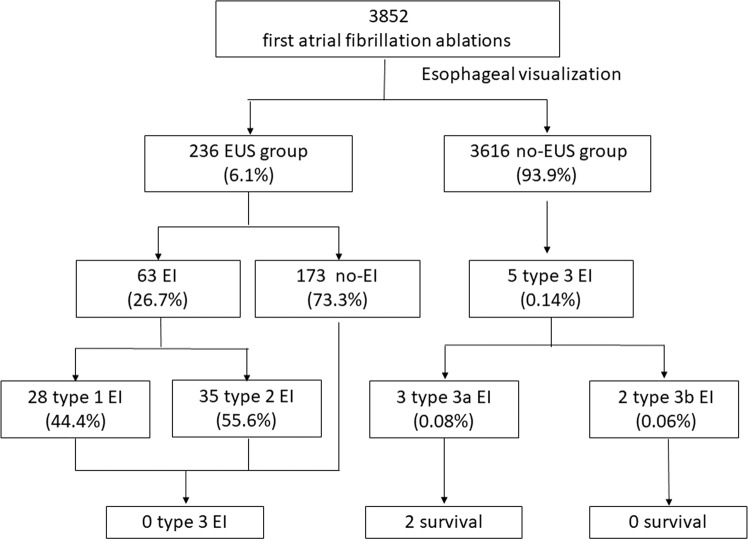
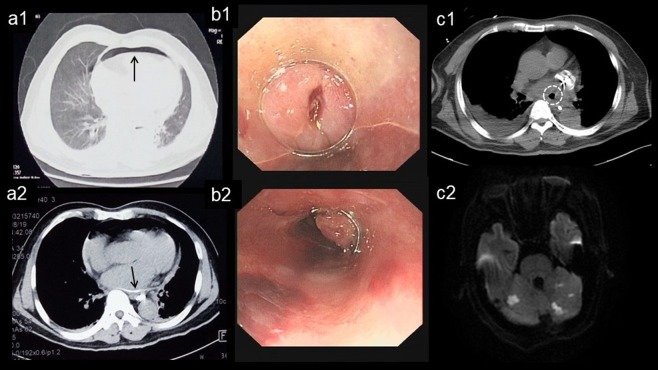
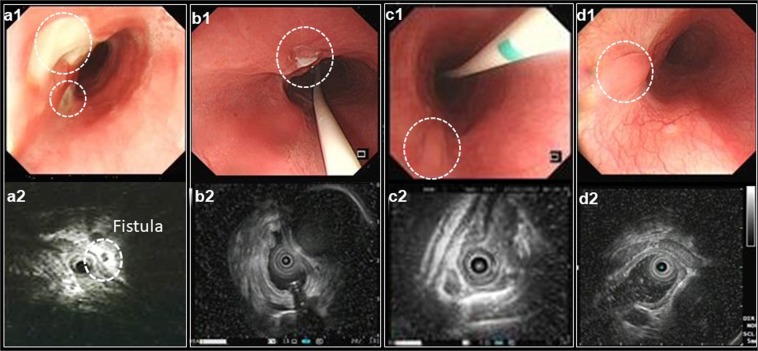
The close proximity of esophagus to the left atrial posterior wall predisposes esophagus to thermal injury during catheter ablation for atrial fibrillation (AF). In this retrospective study, we aimed to investigate risk factors of esophageal injury (EI) caused by catheter ablation for AF. Patients who underwent first-time AF ablation from July 2013 to June 2018 were included. The esophagus was visualized by oral soluble contrast during ablation for all patients and a subset of patients were selected to undergo endoscopic ultrasonography (EUS) to estimate EI post ablation. Degree of EI was categorized as Kansas City classification: type 1: erythema; type 2: ulcers (2a: superficial ulcers; 2b: deep ulcers); type 3: perforation (3a: perforation without communication with the atria; 3b: atrioesophageal fistula [AEF]). Of 3,852 patients, 236 patients (61.5 ± 9.7 years; male, 69%) received EUS (EUS group) and 3616 (63.2 ± 10.9 years; male, 61.1%) without EUS (No-EUS group). In EUS group, EI occurred in 63 patients (type 1 EI in 35 and type 2 EI in 28), and no type 3 EI was observed during follow up. In a multivariable logistic regression analysis, an overlap between the ablation lesion and esophagus was an independent predictor of EI (odds ratio, 21.2; 95% CI: 6.23-72.0; P < 0.001). In No-EUS group, esophagopericardial fistula (EPF; n = 3,0.08%) or AEF (n = 2,0.06%) was diagnosed 4-37 days after ablation. In 3 EPF patients, 2 completely recovered with conservative management and 1 died. Two AEF patients died. Ablation at the vicinity of the esophagus predicts risk of EI. EUS post ablation may prevent the progression of EI and should be considered in management of EI. It remains challenging to identify patients with high risk of EI.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Halbfass, P. et al. Progression From Esophageal Thermal Asymptomatic Lesion to Perforation Complicating Atrial Fibrillation Ablation: A Single-Center Registry. Circ Arrhythm Electrophysiol10, 10.1161/CIRCEP.117.005233 (2017). - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
