

Spinal muscular atrophy diagnosis and carrier screening from genome sequencing data
- PMID: 32066871
- PMCID: PMC7200598
- DOI: 10.1038/s41436-020-0754-0
Spinal muscular atrophy diagnosis and carrier screening from genome sequencing data
Abstract
Purpose: Spinal muscular atrophy (SMA), caused by loss of the SMN1 gene, is a leading cause of early childhood death. Due to the near identical sequences of SMN1 and SMN2, analysis of this region is challenging. Population-wide SMA screening to quantify the SMN1 copy number (CN) is recommended by the American College of Medical Genetics and Genomics.
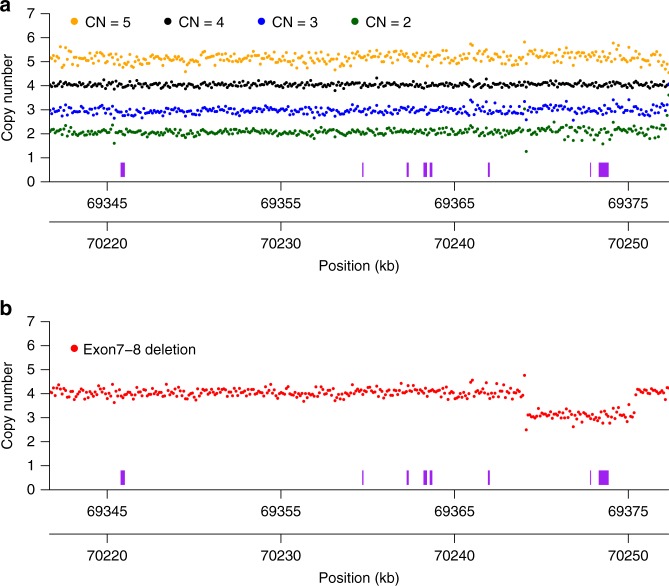
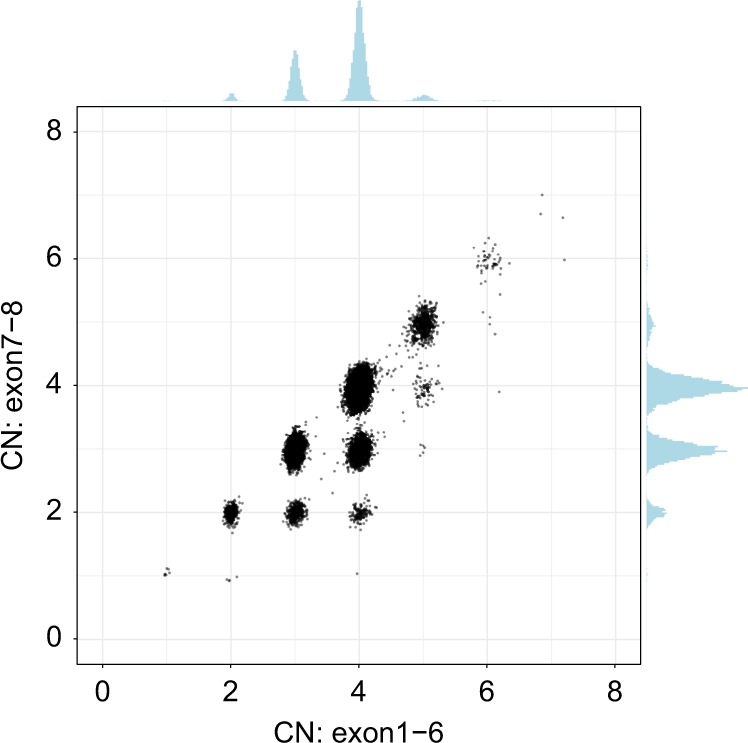
Methods: We developed a method that accurately identifies the CN of SMN1 and SMN2 using genome sequencing (GS) data by analyzing read depth and eight informative reference genome differences between SMN1/2.
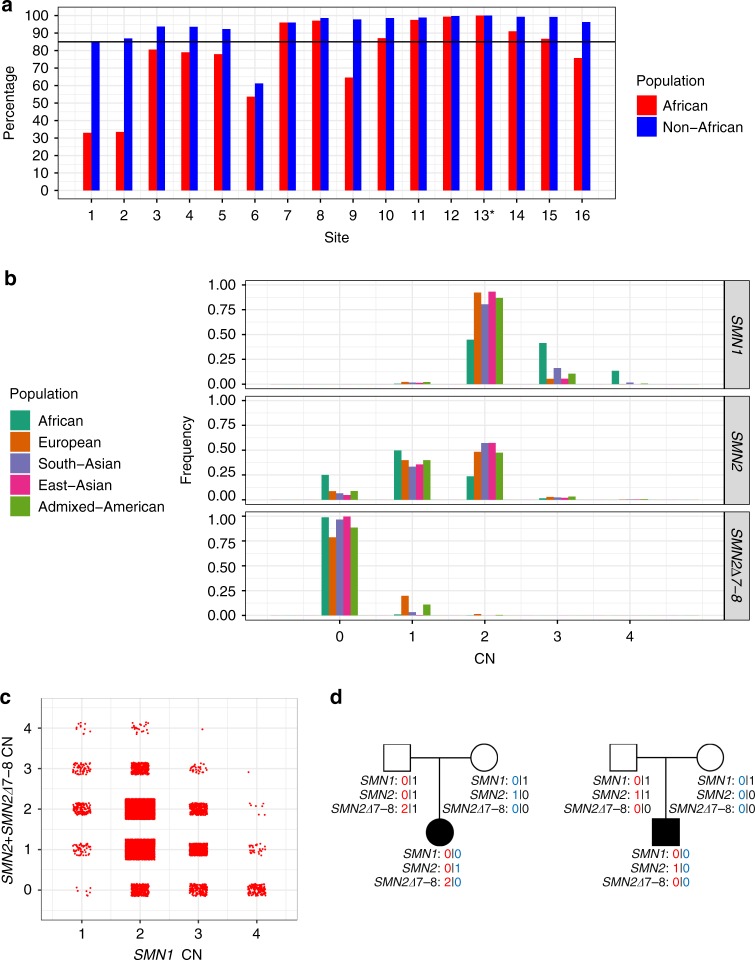
Results: We characterized SMN1/2 in 12,747 genomes, identified 1568 samples with SMN1 gains or losses and 6615 samples with SMN2 gains or losses, and calculated a pan-ethnic carrier frequency of 2%, consistent with previous studies. Additionally, 99.8% of our SMN1 and 99.7% of SMN2 CN calls agreed with orthogonal methods, with a recall of 100% for SMA and 97.8% for carriers, and a precision of 100% for both SMA and carriers.
Conclusion: This SMN copy-number caller can be used to identify both carrier and affected status of SMA, enabling SMA testing to be offered as a comprehensive test in neonatal care and an accurate carrier screening tool in GS sequencing projects.
Keywords: bioinformatics; carrier screening; copy-number analysis; genome sequencing (GS); spinal muscular atrophy (SMA).
Conflict of interest statement
X.C., Z.K., A.C., A.L.H., R.J.T., D.R.B. and M.A.E. are employees of Illumina Inc. The other authors declare no conflicts of interest.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
