

Clinical activity of programmed cell death 1 (PD-1) blockade in never, light, and heavy smokers with non-small-cell lung cancer and PD-L1 expression ≥50
- PMID: 32067682
- PMCID: PMC7545963
- DOI: 10.1016/j.annonc.2019.11.015
Clinical activity of programmed cell death 1 (PD-1) blockade in never, light, and heavy smokers with non-small-cell lung cancer and PD-L1 expression ≥50
Abstract
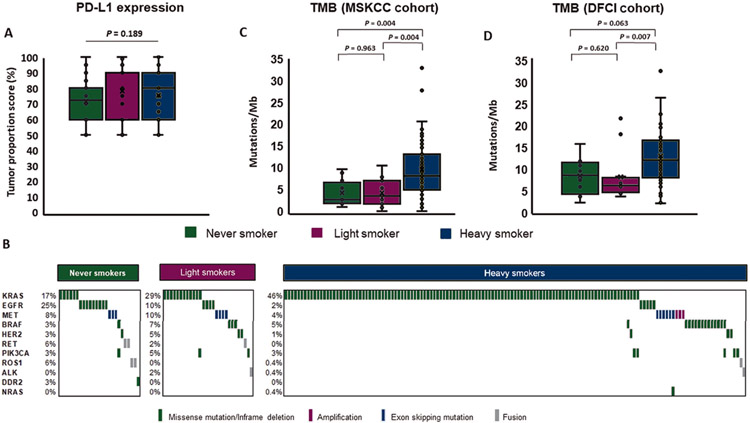
Background: Immune checkpoint inhibitors (ICIs) are standard therapies for patients with advanced non-small-cell lung cancer (NSCLC) and a programmed death-ligand 1 (PD-L1) tumor proportion score (TPS) ≥50%. Tumor mutation burden (TMB) also predicts response to ICIs but is often not available in real time for decision making in the first-line setting. Smoking exposure can be a proxy for TMB in NSCLC. The impact of smoking status on efficacy of PD-1 blockade in NSCLC patients with PD-L1 TPS ≥50% has not been well defined.
Patients and methods: To investigate the relationship between smoking and activity of ICIs in NSCLC, we retrospectively studied 315 patients with NSCLC and PD-L1 TPS ≥50% at five USA academic medical centers. Objective response rates (ORRs), progression-free survival (PFS), and duration of response (DOR) were compared between never (<100 lifetime cigarettes), light (≤10 pack-years), and heavy (>10 pack-years) smokers. A subset of patients underwent next-generation sequencing to estimate TMB.
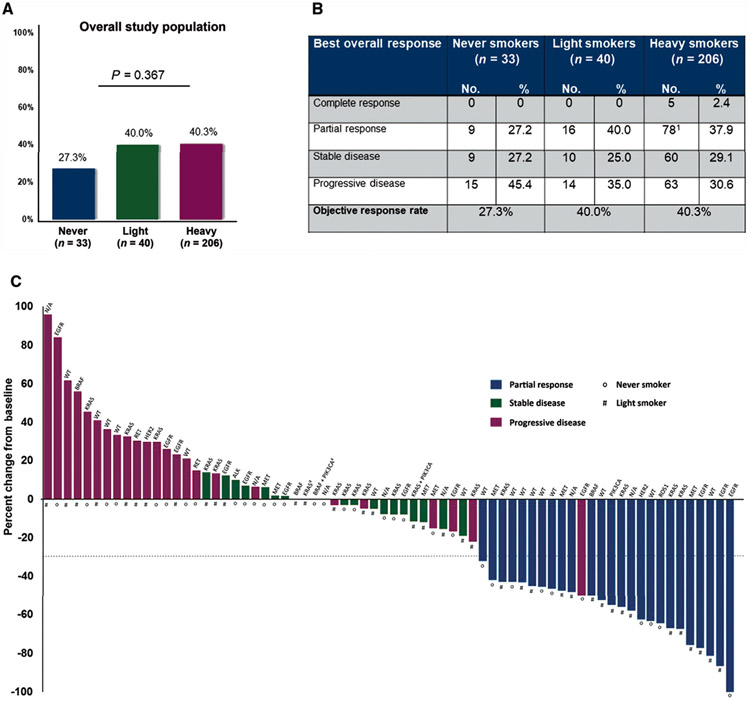
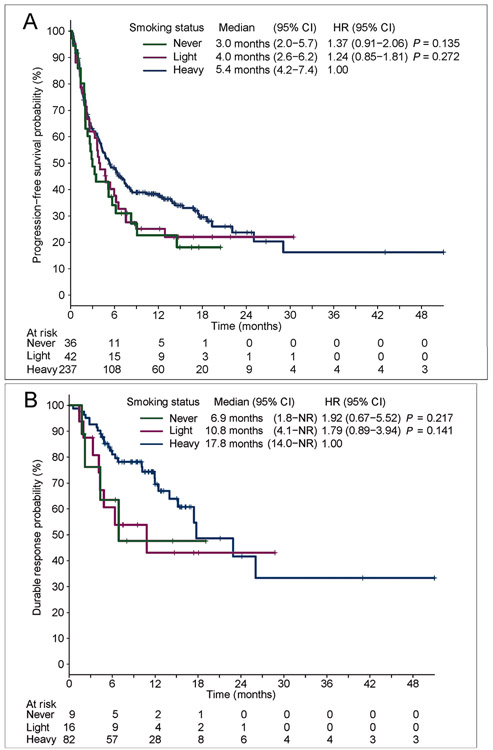
Results: We identified 36 (11%) never, 42 (13%) light, and 237 (75%) heavy smokers with NSCLC and PD-L1 TPS ≥50% treated with ICIs. Objective responses were observed in 27%, 40%, and 40% of never, light, and heavy smokers, respectively (P = 0.180 never versus heavy; P = 1.000 light versus heavy). Median PFS and median DOR were numerically shorter in never and light smokers compared with heavy smokers (PFS 3.0 versus 4.0 versus 5.4 months; median DOR 6.9 versus 10.8 versus 17.8 months), but were not statistically different [PFS: hazard ratio (HR) 1.37, P = 0.135 and HR 1.24, P = 0.272; DOR: HR 1.92, P = 0.217 and HR 1.79, P = 0.141].
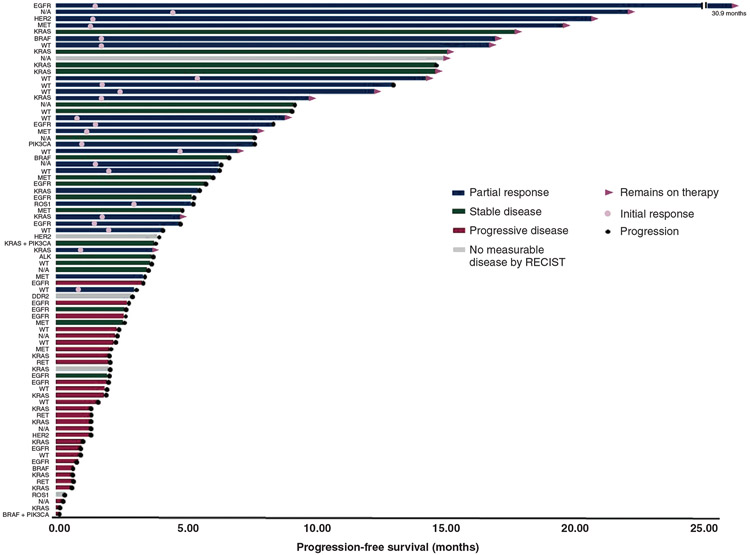
Conclusions: PD-(L)1 inhibitors are associated with antitumor activity in NSCLC with PD-L1 TPS ≥50% regardless of smoking status. Nevertheless, there is a signal of potentially decreased durability among never and light smokers that should be further evaluated. Distinct immunobiologic features may affect initial response versus durability of antitumor immunity to programmed cell death 1 (PD-1) blockade.
Keywords: NSCLC; PD-1 inhibitor; PD-L1 expression; tumor mutation burden.
Copyright © 2019 The Authors. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Disclosure JFG: consultant or received honoraria from Bristol-Myers Squibb, Genentech/Roche, Ariad/Takeda, Loxo, Pfizer, Incyte, Novartis, Merck, Agios, Amgen, Regeneron, Oncorus, Array, Jounce, and Clovis Oncology, research support from Novartis, Genentech/Roche, and Ariad/Takeda, and institutional research support from Bristol-Myers Squibb, Tesaro, Moderna, Blueprint, Jounce, Array Biopharma, Merck, Adaptimmune, Novartis, and Alexo. JAR: consultant and equity in Genprex. BPL: Elsevier textbook author and editor, and receives royalties for his work. KA: consultant or received honoraria from AstraZeneca and Jackson Laboratory. JA: owns stock in Merck, Pfizer, and Thermo Fischer Scientific. MMK: consultant for Merimack Pharmaceuticals and H3 Biomedicine. ATS: consultant or received honoraria from Pfizer, Novartis, Chugai, Genentech/Roche, Ariad/Takeda, Ignyta, LOXO, Blueprint Medicines, KSQ Therapeutics, Daiichi Sankyo, EMD Serono, Taiho Pharmaceutical, TP Therapeutics, Bayer, Foundation Medicine, Guardant, and Natera. Institutional research funding from: Pfizer, Novartis, Roche/Genentech, Ariad, Ignyta, and TP Therapeutics. MMA: consultant or received honoraria from Merck, Bristol-Myers Squibb, Genentech, AstraZeneca, Nektar, Blueprint, Maverick, and Syndax and research support from Bristol-Myers Squibb, AstraZeneca, Lilly, and Genentech. MDH: has received research funding from Bristol-Myers Squibb; is a paid consultant to Merck, Bristol-Myers Squibb, AstraZeneca, Genentech/Roche, Nektar, Syndax, Mirati, Shattuck Labs, and Immunai; has received travel support/honoraria from AztraZeneca and BMS; and a patent has been filed by MSK related to the use of tumor mutation burden to predict response to immunotherapy (PCT/US2015/062208), which has received licensing fees from PGDx. The remaining authors have no conflicts of interest to disclose.
Figures
References
-
- Reck M, Rodríguez-Abreu D, Robinson AG, et al. Pembrolizumab versus chemotherapy for PD-L1-positive non-small-cell lung cancer. N Engl J Med. 2016;375:1823–1833. - PubMed
-
- Gettinger S, Horn L, Jackman D, et al. Five-year follow-up of nivolumab in previously treated advanced non-small-cell lung cancer: Results from the CA209-003 study. J Clin Oncol. 2018;36:1675–1684. - PubMed
-
- Rizvi H, Sanchez-Vega F, La K, et al. Molecular determinants of response to anti-programmed cell death (PD)-1 and anti-programmed death-ligand 1 (PD-L1) blockade in patients with non-small-cell lung cancer profiled with targeted next-generation sequencing. J Clin Oncol. 2018;36:633–641. - PMC - PubMed
-
- Garon EB, Rizvi NA, Hui R, et al. Pembrolizumab for the treatment of non-small-cell lung cancer. N Engl J Med. 2015;372:2018–2028. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
