

Amyloid-β Positivity Predicts Cognitive Decline but Cognition Predicts Progression to Amyloid-β Positivity
- PMID: 32067693
- PMCID: PMC7166153
- DOI: 10.1016/j.biopsych.2019.12.021
Amyloid-β Positivity Predicts Cognitive Decline but Cognition Predicts Progression to Amyloid-β Positivity
Abstract
Background: Stage 1 of the National Institute on Aging-Alzheimer's Association's proposed Alzheimer's disease continuum is defined as amyloid-β (Aβ) positive but cognitively normal. Identifying at-risk individuals before Aβ reaches pathological levels could have great benefits for early intervention. Although Aβ levels become abnormal long before severe cognitive impairments appear, increasing evidence suggests that subtle cognitive changes may begin early, potentially before Aβ surpasses the threshold for abnormality. We examined whether baseline cognitive performance would predict progression from normal to abnormal levels of Aβ.
Methods: We examined the association of baseline cognitive composites (Preclinical Alzheimer Cognitive Composite, Alzheimer's Disease Neuroimaging Initiative (ADNI) memory factor composite) with progression to Aβ positivity in 292 nondemented, Aβ-negative ADNI participants. Additional analyses included continuous cerebrospinal fluid biomarker levels to examine the effects of subthreshold pathology.
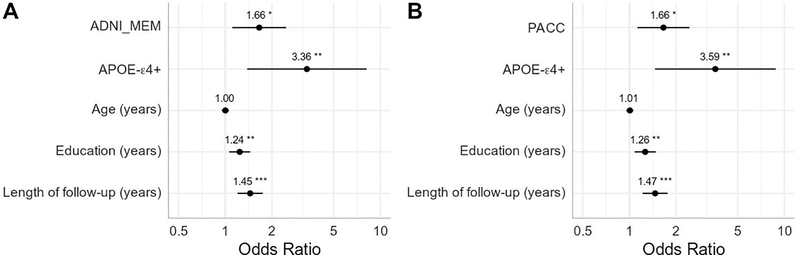
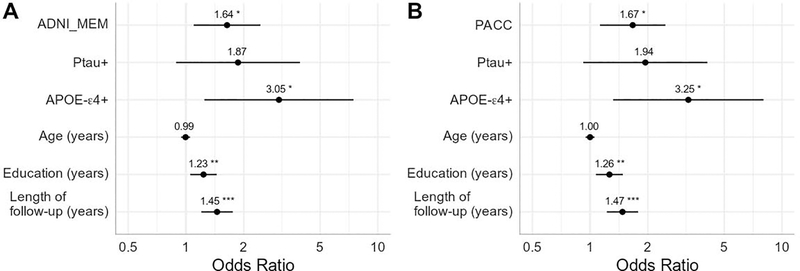
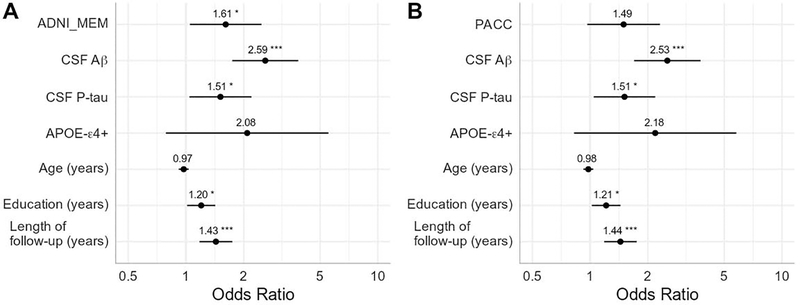
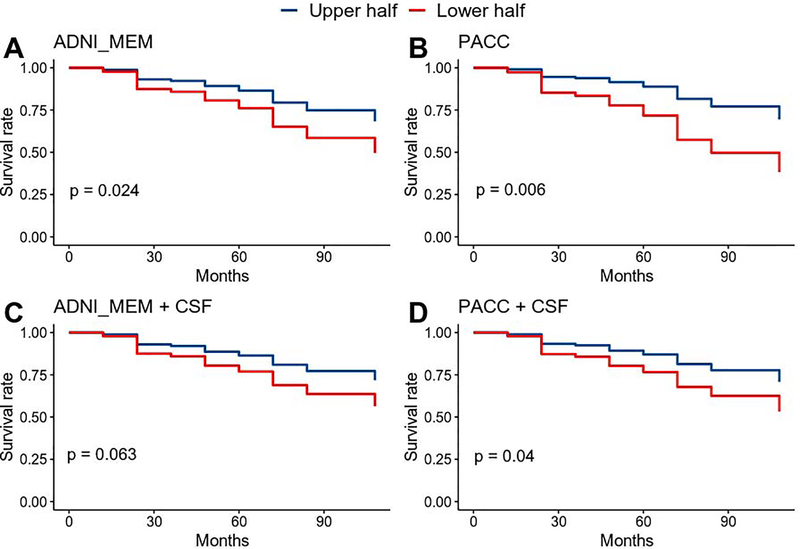
Results: Forty participants progressed to Aβ positivity during follow-up. Poorer baseline performance on both cognitive measures was significantly associated with increased odds of progression. More abnormal levels of baseline cerebrospinal fluid phosphorylated tau and subthreshold Aβ were associated with increased odds of progression to Aβ positivity. Nevertheless, baseline ADNI memory factor composite performance predicted progression even after controlling for baseline biomarker levels and APOE genotype (Preclinical Alzheimer Cognitive Composite was trend level). Survival analyses were largely consistent: controlling for baseline biomarker levels, baseline Preclinical Alzheimer Cognitive Composite still significantly predicted progression time to Aβ positivity (ADNI memory factor composite was trend level).
Conclusions: The possibility of intervening before Aβ reaches pathological levels is of obvious benefit. Low-cost, noninvasive cognitive measures can be informative for determining who is likely to progress to Aβ positivity, even after accounting for baseline subthreshold biomarker levels.
Keywords: AD; Alzheimer’s disease; Amyloid accumulation; Biomarker trajectories; Cognition; MCI; Mild cognitive impairment; β-amyloid.
Copyright © 2020 Society of Biological Psychiatry. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
DISCLOSURES
The authors report no biomedical financial interests or potential conflicts of interest.
Figures
Comment in
-
Amyloid Positivity as a Risk Factor for Memory Decline and Lower Memory Performance as an Indicator of Conversion to Amyloid Positivity: Chicken and Egg.Biol Psychiatry. 2020 May 1;87(9):782-784. doi: 10.1016/j.biopsych.2020.02.006. Biol Psychiatry. 2020. PMID: 32299580 Free PMC article. No abstract available.
References
-
- Villemagne VL, Burnham S, Bourgeat P, Brown B, Ellis KA, Salvado O, et al. (2013): Amyloid beta deposition, neurodegeneration, and cognitive decline in sporadic Alzheimer’s disease: a prospective cohort study. Lancet Neurol. 12:357–367. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
