

Predictive Accuracy of a Polygenic Risk Score Compared With a Clinical Risk Score for Incident Coronary Heart Disease
- PMID: 32068817
- PMCID: PMC7042849
- DOI: 10.1001/jama.2019.21782
Predictive Accuracy of a Polygenic Risk Score Compared With a Clinical Risk Score for Incident Coronary Heart Disease
Abstract
Importance: Polygenic risk scores comprising millions of single-nucleotide polymorphisms (SNPs) could be useful for population-wide coronary heart disease (CHD) screening.
Objective: To determine whether a polygenic risk score improves prediction of CHD compared with a guideline-recommended clinical risk equation.
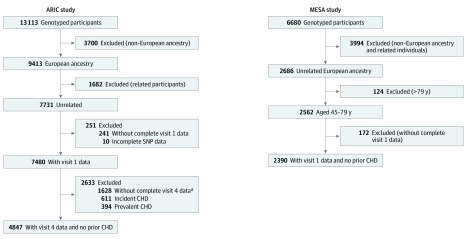
Design, setting, and participants: A retrospective cohort study of the predictive accuracy of a previously validated polygenic risk score was assessed among 4847 adults of white European ancestry, aged 45 through 79 years, participating in the Atherosclerosis Risk in Communities (ARIC) study and 2390 participating in the Multi-Ethnic Study of Atherosclerosis (MESA) from 1996 through December 31, 2015, the final day of follow-up. The performance of the polygenic risk score was compared with that of the 2013 American College of Cardiology and American Heart Association pooled cohort equations.
Exposures: Genetic risk was computed for each participant by summing the product of the weights and allele dosage across 6 630 149 SNPs. Weights were based on an international genome-wide association study.
Main outcomes and measures: Prediction of 10-year first CHD events (including myocardial infarctions, fatal coronary events, silent infarctions, revascularization procedures, or resuscitated cardiac arrest) assessed using measures of model discrimination, calibration, and net reclassification improvement (NRI).
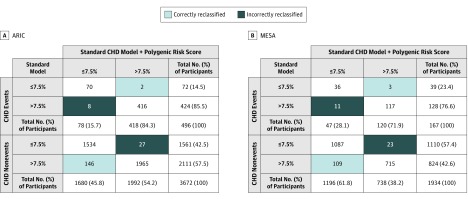
Results: The study population included 4847 adults from the ARIC study (mean [SD] age, 62.9 [5.6] years; 56.4% women) and 2390 adults from the MESA cohort (mean [SD] age, 61.8 [9.6] years; 52.2% women). Incident CHD events occurred in 696 participants (14.4%) and 227 participants (9.5%), respectively, over median follow-up of 15.5 years (interquartile range [IQR], 6.3 years) and 14.2 (IQR, 2.5 years) years. The polygenic risk score was significantly associated with 10-year CHD incidence in ARIC with hazard ratios per SD increment of 1.24 (95% CI, 1.15 to 1.34) and in MESA, 1.38 (95% CI, 1.21 to 1.58). Addition of the polygenic risk score to the pooled cohort equations did not significantly increase the C statistic in either cohort (ARIC, change in C statistic, -0.001; 95% CI, -0.009 to 0.006; MESA, 0.021; 95% CI, -0.0004 to 0.043). At the 10-year risk threshold of 7.5%, the addition of the polygenic risk score to the pooled cohort equations did not provide significant improvement in reclassification in either ARIC (NRI, 0.018, 95% CI, -0.012 to 0.036) or MESA (NRI, 0.001, 95% CI, -0.038 to 0.076). The polygenic risk score did not significantly improve calibration in either cohort.
Conclusions and relevance: In this analysis of 2 cohorts of US adults, the polygenic risk score was associated with incident coronary heart disease events but did not significantly improve discrimination, calibration, or risk reclassification compared with conventional predictors. These findings suggest that a polygenic risk score may not enhance risk prediction in a general, white middle-aged population.
Conflict of interest statement
Figures
Comment in
-
Do Polygenic Risk Scores Improve Patient Selection for Prevention of Coronary Artery Disease?JAMA. 2020 Feb 18;323(7):614-615. doi: 10.1001/jama.2019.21667. JAMA. 2020. PMID: 32068803 No abstract available.
References
-
- Benjamin EJ, Muntner P, Alonso A, et al. ; American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee . Heart disease and stroke statistics-2019 update: a report from the American Heart Association. Circulation. 2019;139(10):e56-e528. doi: 10.1161/CIR.0000000000000659 - DOI - PubMed
-
- Goff DC Jr, Lloyd-Jones DM, Bennett G, et al. ; American College of Cardiology/American Heart Association Task Force on Practice Guidelines . 2013 ACC/AHA guideline on the assessment of cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129(25)(suppl 2):S49-S73. doi: 10.1161/01.cir.0000437741.48606.98 - DOI - PubMed
