

Predictive Accuracy of a Polygenic Risk Score-Enhanced Prediction Model vs a Clinical Risk Score for Coronary Artery Disease
- PMID: 32068818
- PMCID: PMC7042853
- DOI: 10.1001/jama.2019.22241
Predictive Accuracy of a Polygenic Risk Score-Enhanced Prediction Model vs a Clinical Risk Score for Coronary Artery Disease
Abstract
Importance: The incremental value of polygenic risk scores in addition to well-established risk prediction models for coronary artery disease (CAD) is uncertain.
Objective: To examine whether a polygenic risk score for CAD improves risk prediction beyond pooled cohort equations.
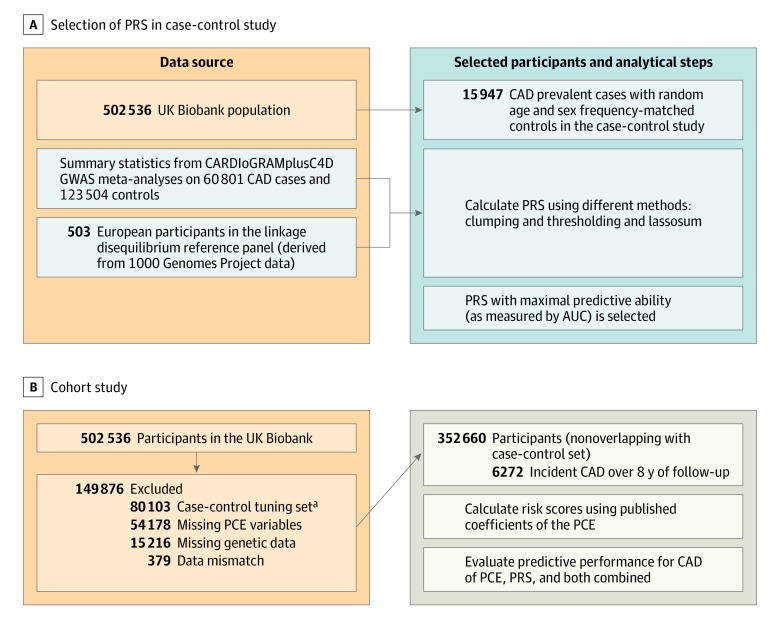
Design, setting, and participants: Observational study of UK Biobank participants enrolled from 2006 to 2010. A case-control sample of 15 947 prevalent CAD cases and equal number of age and sex frequency-matched controls was used to optimize the predictive performance of a polygenic risk score for CAD based on summary statistics from published genome-wide association studies. A separate cohort of 352 660 individuals (with follow-up to 2017) was used to evaluate the predictive accuracy of the polygenic risk score, pooled cohort equations, and both combined for incident CAD.
Exposures: Polygenic risk score for CAD, pooled cohort equations, and both combined.
Main outcomes and measures: CAD (myocardial infarction and its related sequelae). Discrimination, calibration, and reclassification using a risk threshold of 7.5% were assessed.
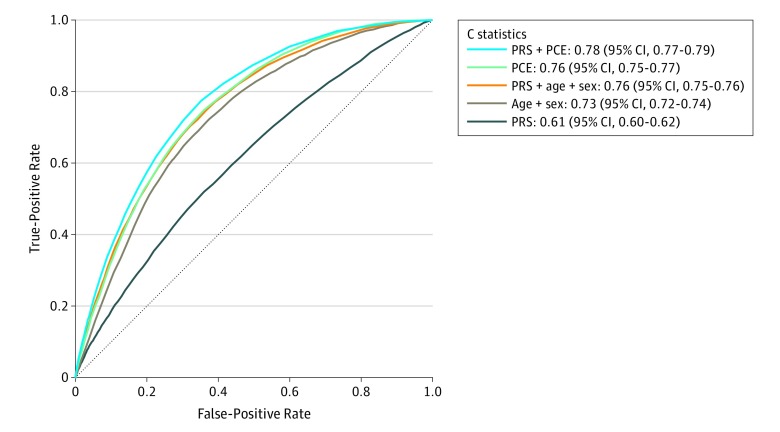
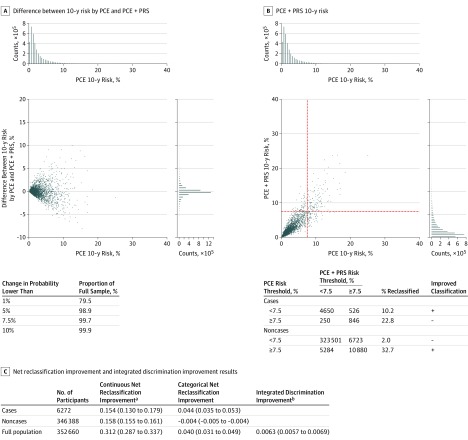
Results: In the cohort of 352 660 participants (mean age, 55.9 years; 205 297 women [58.2%]) used to evaluate the predictive accuracy of the examined models, there were 6272 incident CAD events over a median of 8 years of follow-up. CAD discrimination for polygenic risk score, pooled cohort equations, and both combined resulted in C statistics of 0.61 (95% CI, 0.60 to 0.62), 0.76 (95% CI, 0.75 to 0.77), and 0.78 (95% CI, 0.77 to 0.79), respectively. The change in C statistic between the latter 2 models was 0.02 (95% CI, 0.01 to 0.03). Calibration of the models showed overestimation of risk by pooled cohort equations, which was corrected after recalibration. Using a risk threshold of 7.5%, addition of the polygenic risk score to pooled cohort equations resulted in a net reclassification improvement of 4.4% (95% CI, 3.5% to 5.3%) for cases and -0.4% (95% CI, -0.5% to -0.4%) for noncases (overall net reclassification improvement, 4.0% [95% CI, 3.1% to 4.9%]).
Conclusions and relevance: The addition of a polygenic risk score for CAD to pooled cohort equations was associated with a statistically significant, yet modest, improvement in the predictive accuracy for incident CAD and improved risk stratification for only a small proportion of individuals. The use of genetic information over the pooled cohort equations model warrants further investigation before clinical implementation.
Conflict of interest statement
Figures
Comment in
References
-
- Arnett DK, Blumenthal RS, Albert MA, et al. 2019 ACC/AHA guideline on the primary prevention of cardiovascular disease: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2019;74(10):e177-e232. doi: 10.1016/j.jacc.2019.03.010 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
