

Effect of the Xpert MTB/RIF on the detection of pulmonary tuberculosis cases and rifampicin resistance in Shanghai, China
- PMID: 32070292
- PMCID: PMC7029590
- DOI: 10.1186/s12879-020-4871-9
Effect of the Xpert MTB/RIF on the detection of pulmonary tuberculosis cases and rifampicin resistance in Shanghai, China
Abstract
Background: Xpert MTB/RIF (Xpert) is an automated molecular test recommended by World Health Organization (WHO) for diagnosis of tuberculosis (TB). This study evaluated the effect of Xpert implementation on the detection of pulmonary TB (PTB) and rifampicin-resistant TB (RR-TB) cases in Shanghai, China.
Methods: Xpert was routinely implemented in 2018 for all presumptive PTB patients. All PTB patients above 15 years-old identified within the Provincial TB Control Program during the first half of each of 2017 and 2018, were enrolled to compare the difference in proportions of bacteriological confirmation, patients with drug susceptibility test (DST) results for rifampicin (ie, DST coverage) and RR-TB detection before and after Xpert's implementation.
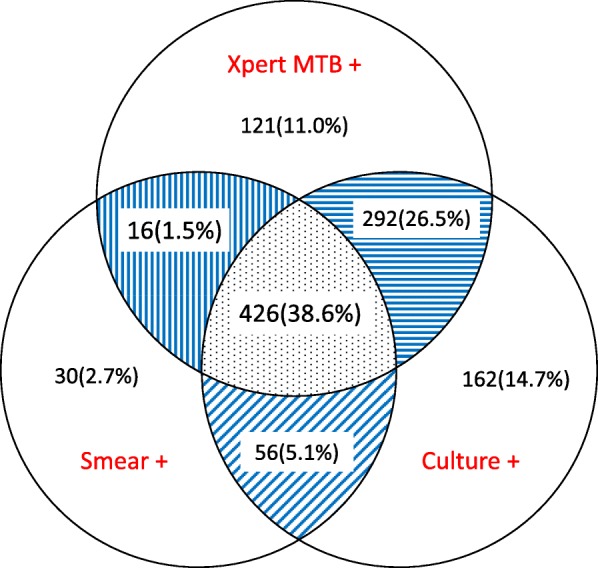
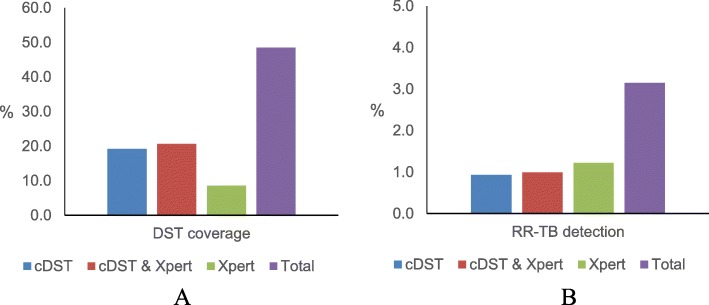
Results: A total of 6047 PTB patients were included in the analysis with 1691 tested by Xpert in 2018. Percentages of bacteriological confirmation, DST coverage and RR-TB detection in 2017 and 2018 were 50% vs. 59%, 36% vs. 49% and 2% vs. 3%, respectively (all p-values < 0.05). Among 1103 PTB patients who completed sputum smear, culture and Xpert testing in 2018, Xpert detected an additional 121 (11%) PTB patients who were negative by smear and culture, but missed 248 (23%) smear and/or culture positive patients. Besides, it accounted for an increase of 9% in DST coverage and 1% in RR-TB detection. The median time from first visit to a TB hospital to RR-TB detection was 62 days (interquartile range -IQR 48-84.2) in 2017 vs. 9 days (IQR 2-45.7) in 2018 (p-value < 0.001). In the multivariate model, using Xpert was associated with decreased time to RR-TB detection (adjusted hazard ratio = 4.62, 95% confidence interval: 3.18-6.71).
Conclusions: Integrating Xpert with smear, culture and culture-based DST in a routine setting significantly increased bacteriological confirmation, DST coverage and RR-TB detection with a dramatic reduction in the time to RR-TB diagnosis in Shanghai, China. Our findings can be useful for other regions that attempt to integrate Xpert into routine PTB and RR-TB case-finding cascade. Further study should focus on the identification and elimination of operational level challenges to fully utilize the benefit of rapid diagnosis by Xpert.
Keywords: Delay; Rifampicin resistant; SORT IT; TB; Tuberculosis; Xpert MTB/RIF.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- World Health Organization. Global tuberculosis report 2018. Geneva: World Health Organization; 2018.
-
- Implementing tuberculosis diagnostics . Policy framework. Geneva: World Health Organization; 2015.
-
- World Health Organization. Automated real-time nucleic acid amplification technology for rapid and simultaneous detection of tuberculosis and rifampicin resistance: Xpert MTB/RIF assay for the diagnosis of pulmonary and extrapulmonary TB in adults and children: policy update. Geneva: World Health Organization; 2013. - PubMed
MeSH terms
Substances
Grants and funding
- 2018ZX10715012/Ministry of Science and Technology of the People's Republic of China
- 2017YFD0500301/Ministry of Science and Technology of the People's Republic of China
- 2017ZX10201302-006-002/Ministry of Science and Technology of the People's Republic of China
- 81872679/National Natural Science Foundation of China
LinkOut - more resources
Full Text Sources
Medical
